




Paediatric Respiratory & ENT Emergencies | Medical Revision
Master childhood asthma, bronchiolitis, pneumonia, croup, and cystic fibrosis. UKMLA-aligned revision with practice SBA questions and clinical pearls.
45–60 min session
Session 1
Paediatric Respiratory &<br>ENT Emergencies
Common Conditions & Clinical Reasoning
Asthma
Bronchiolitis
Pneumonia
Croup
Epiglottitis
Cystic Fibrosis
Learning Objectives
Session 1
Diagnose and classify childhood asthma
Recognise and manage acute asthma exacerbations
Diagnose bronchiolitis and identify admission criteria
Differentiate viral from bacterial pneumonia
Distinguish croup from epiglottitis in examinations and OSCEs
Understand the diagnosis and management of cystic fibrosis
Apply UKMLA-style clinical reasoning to paediatric respiratory presentations
Learning Objectives
Asthma
Bronchiolitis
Pneumonia
Croup/Epiglottitis
Cystic Fibrosis
Session Overview
SECTION 1
Asthma
SECTION 2
Bronchiolitis
SECTION 3
Pneumonia / LRTI
SECTION 4
Croup vs Epiglottitis
SECTION 5
Cystic Fibrosis
Format:
Question <span style="color:#006670;font-weight:800;margin:0 4px;">→</span> Discussion <span style="color:#006670;font-weight:800;margin:0 4px;">→</span> Key Learning Point
~1 MCQ every 2–3 slides
UKMLA Aligned <span style="margin: 0 8px; opacity: 0.5;">|</span> Active Recall <span style="margin: 0 8px; opacity: 0.5;">|</span> Case-Based Learning
01
SECTION 1
ASTHMA
Epidemiology · Diagnosis · Management · Acute Exacerbations
Epidemiology
Pathophysiology
Diagnosis
BTS/SIGN Steps
Acute Management
Severity Classification
Asthma: Epidemiology & Pathophysiology
Epidemiology
Most common chronic childhood condition in UK
Affects <span style="font-weight: 800; color: #006670;">~1 in 11 children</span>
Peak onset: <span style="font-weight: 800; color: #006670;">5–10 years</span>
<span style="font-weight: 800; color: #006670;">2× more common</span> in boys (pre-puberty)
Major cause of school absence & hospital admissions
1,200+ deaths/year in UK (mostly preventable)
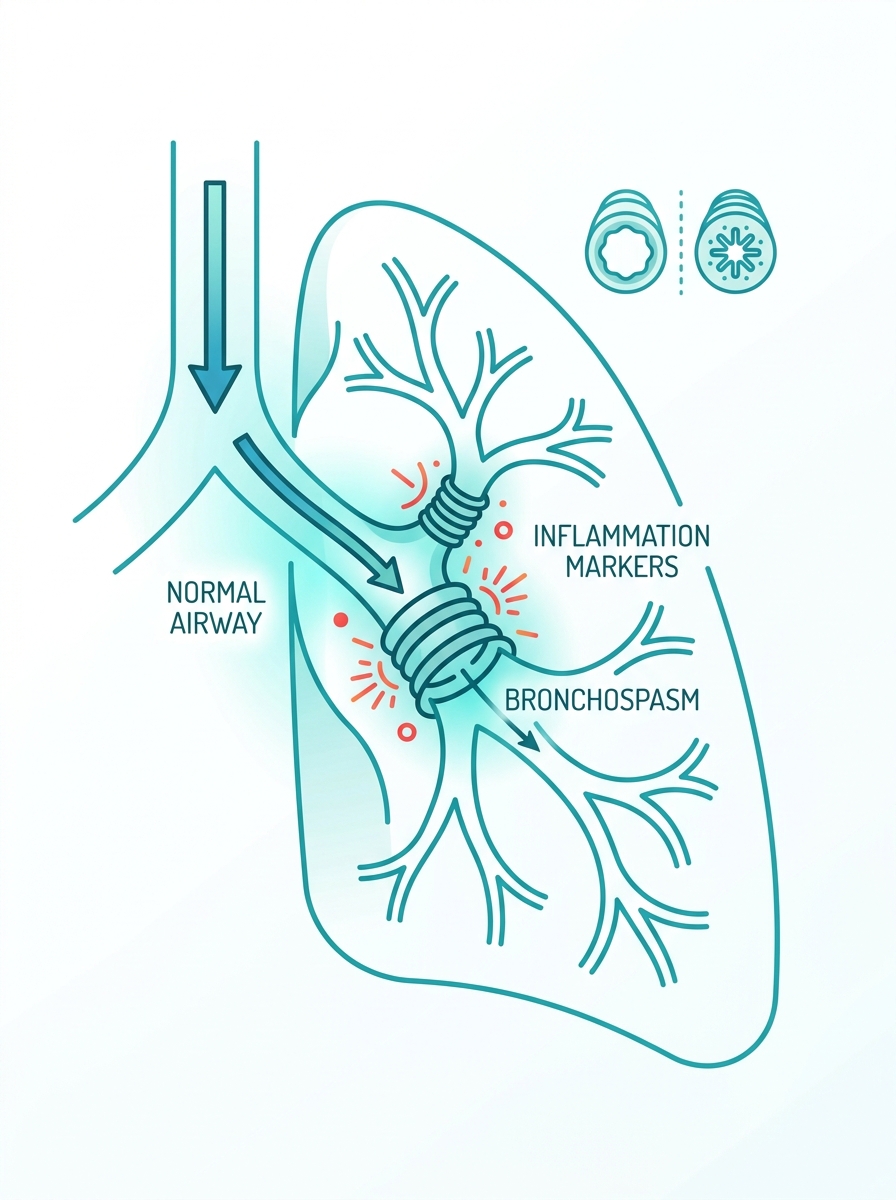
Pathophysiology
<span style="font-weight: 800; color: #0D2C4E;">Chronic airway inflammation</span> (eosinophils, mast cells, T-lymphocytes)
Airway hyperresponsiveness
Reversible bronchoconstriction
<span style="font-weight: 800; color: #0D2C4E;">Triggers:</span> viral URTI, allergens, exercise, cold air, smoke
Remodelling with repeated exacerbations
Exam Pearl
<span style="font-weight: 800; color: #B4781A;">Atopic triad = Asthma + Eczema + Allergic Rhinitis.</span> Ask about family history! Atopy is a key risk factor.
Diagnosing Asthma in Children
Clinical Features
Main Symptoms
Wheeze, cough (worse at night), breathlessness, chest tightness
Diurnal Variation
Symptoms typically observed to be worse in mornings and nights
Episodic Triggers
Often triggered by exercise, viral URTIs, or environmental allergens
Reversibility
Clear positive symptomatic response to bronchodilator (salbutamol)
>5 Years Old
<strong>Spirometry:</strong> FEV1/FVC ratio <70%
<strong>Bronchodilator reversibility:</strong> ≥12% increase in FEV1
<strong>FeNO</strong> >35 ppb supports diagnosis
<strong>Peak flow variability</strong> >20%
<5 Years Old
<strong>Clinical diagnosis only</strong>
No reliable spirometry options
Trial of salbutamol MDI + spacer
Watchful waiting acceptable
Response to treatment confirms suspicion
<strong>Diagnostic Pearl:</strong> Under-5s are diagnosed clinically — spirometry is NOT reliable. Salbutamol response is the key diagnostic tool.
SBA QUESTION 1
A 7-year-old boy is referred to the paediatric outpatient clinic with a 6-month history of nocturnal cough and wheeze. His mother has asthma. Spirometry shows FEV1/FVC = 64%. After salbutamol, FEV1 increases by 14%. He has mild eczema.
What is the most appropriate next step in management?
Start high-dose inhaled corticosteroid immediately
Diagnose asthma and start BTS Step 1 — low-dose ICS
Arrange FeNO measurement before confirming diagnosis
Refer to respiratory paediatrician without starting treatment
Trial of 8 weeks montelukast
Think before you click… What criteria confirm asthma here?
Answer on next slide →
ANSWER: B
Correct Answer: B — Diagnose asthma and start BTS Step 1 (low-dose ICS)
EXPLANATION
FEV1/FVC <70% = obstructive pattern
Bronchodilator reversibility ≥12% = positive
Clinical features: nocturnal cough, wheeze, atopic history
This meets diagnostic criteria → start treatment
EXAM PEARL
BTS/SIGN Step 1 = Low-dose ICS (e.g. beclometasone 200mcg/day). NEVER start Step 2 without trialling Step 1 first.
WHY THE OTHERS ARE WRONG
High-dose ICS not appropriate as first step — start low-dose
FeNO is supportive but not required when spirometry is diagnostic
No need for specialist referral when diagnosis is confirmed
Montelukast is not first-line treatment in asthma
BTS/SIGN Guidelines
Stepwise Management of Childhood Asthma
High-dose ICS + LABA
+ consider oral corticosteroids or biologics — Specialist centre
Medium-dose ICS + LABA
Refer to respiratory paediatrician
Low-dose ICS + LABA (salmeterol)
Consider LTRA (montelukast) if LABA not tolerated
Low-dose ICS
Beclometasone 200mcg/day OR equivalent
SABA PRN
Salbutamol MDI + spacer as needed
Review inhaler technique and adherence BEFORE stepping up! Most 'uncontrolled asthma' = poor technique.
Asthma Guidelines
Acute Asthma: Severity Classification
Clinical Feature
MILD
MODERATE
SEVERE
LIFE-THREATENING
SpO₂
≥94%
≥92%
<92%
<92% + exhausted
PEFR
>50% best
33–50% best
<33% best
Too exhausted to perform
Speech
Normal sentences
Short sentences
Words only
Silent chest
RR
Normal for age
Slightly raised
Significantly raised
Bradypnoea (pre-arrest)
HR
Normal
Mild tachycardia
Significant tachycardia
Bradycardia
Accessory muscles
None
Mild
Marked
Paradoxical breathing
Consciousness
Alert
Alert
Agitated/distressed
Drowsy/confused
Life-Threatening Features
Silent chest + SpO₂ <92% + Cyanosis + Poor respiratory effort + Exhaustion + Altered consciousness
Immediate senior review + IV magnesium + ICU alert
Acute Asthma: Emergency Management Algorithm
Child presents with acute wheeze/breathlessness <span style="margin: 0 15px; color: #94A3B8;">→</span> <span style="font-weight: 500; opacity: 0.9;">Assess severity</span>
MILD
<ul style="margin: 0; padding-left: 24px; color: #1E293B; font-size: 22px; line-height: 1.4; font-weight: 500;"> <li style="margin-bottom: 20px;">Salbutamol 2–4 puffs MDI + spacer PRN</li> <li style="margin-bottom: 20px;">Review in 1 hour</li> <li style="margin-bottom: 0;">Discharge home with written action plan</li> </ul>
MODERATE
<ul style="margin: 0; padding-left: 24px; color: #1E293B; font-size: 22px; line-height: 1.4; font-weight: 500;"> <li style="margin-bottom: 20px;"><strong style="color: #D97706;">O<sub style="font-size: 16px; bottom: -2px; position: relative;">2</sub></strong> if SpO<sub style="font-size: 16px; bottom: -2px; position: relative;">2</sub> < 94%</li> <li style="margin-bottom: 20px;">Salbutamol 10 puffs MDI + spacer <br><span style="color: #64748B; font-size: 18px; font-weight: 700;">OR</span> 2.5mg nebuliser q20min x3</li> <li style="margin-bottom: 20px;">Oral prednisolone 1–2mg/kg (max 40mg) for 3–5 days</li> <li style="margin-bottom: 0;">Reassess after 1 hr → <strong style="color: #D97706;">Admit if not improving</strong></li> </ul>
SEVERE
<ul style="margin: 0; padding-left: 24px; color: #1E293B; font-size: 22px; line-height: 1.4; font-weight: 500;"> <li style="margin-bottom: 20px;">High-flow <strong style="color: #DC2626;">O<sub style="font-size: 16px; bottom: -2px; position: relative;">2</sub></strong> via non-rebreather mask</li> <li style="margin-bottom: 20px;">Back-to-back salbutamol nebs q20min</li> <li style="margin-bottom: 20px;">Ipratropium bromide 250mcg neb (x3 doses)</li> <li style="margin-bottom: 20px;">IV/oral prednisolone</li> <li style="margin-bottom: 0;">IV MgSO<sub style="font-size: 16px; bottom: -2px; position: relative;">4</sub> 40mg/kg if poor response → <strong style="color: #DC2626;">ADMIT</strong></li> </ul>
LIFE-THREATENING
<ul style="margin: 0; padding-left: 24px; color: #1E293B; font-size: 22px; line-height: 1.4; font-weight: 500;"> <li style="margin-bottom: 20px;"><strong style="color: #7F1D1D;">Call for help / Senior review / Anaesthetics</strong></li> <li style="margin-bottom: 20px;">High-flow <strong style="color: #7F1D1D;">O<sub style="font-size: 16px; bottom: -2px; position: relative;">2</sub></strong></li> <li style="margin-bottom: 20px;">IV salbutamol + IV MgSO<sub style="font-size: 16px; bottom: -2px; position: relative;">4</sub></li> <li style="margin-bottom: 20px;">ICU referral</li> <li style="margin-bottom: 0;">Consider IV aminophylline</li> </ul>
<strong style="color: #006670;">UKMLA</strong> Curriculum Aligned | BTS/SIGN | NICE Guidance
SBA QUESTION 2
A 9-year-old girl with known asthma is brought to the ED by her parents. She is using accessory muscles, can only speak in words, and her SpO2 is 90% on air.
Her PEFR is 28% of predicted best. She has already received salbutamol 10 puffs via spacer 30 minutes ago with minimal improvement.
What is the single most appropriate NEXT step in management?
Think before you click
What severity is this? What does PEFR 28% tell you?
Repeat salbutamol 10 puffs via spacer and reassess in 20 minutes
Give nebulised salbutamol + ipratropium bromide and IV/oral prednisolone
Administer IV magnesium sulphate 40mg/kg immediately
Arrange urgent CXR to exclude pneumothorax
Start IV aminophylline infusion
Answer on next slide →
ANSWER: B
Nebulised salbutamol + ipratropium + prednisolone
<b>PEFR 28%</b> = SEVERE (< 33% predicted)
<b>SpO<sub>2</sub> 90%</b> = below threshold → needs O<sub>2</sub>
<b>Words only</b> = SEVERE asthma
<b>SEVERE management:</b> back-to-back nebs salbutamol + ipratropium x3, oral/IV prednisolone, O<sub>2</sub> to maintain SpO<sub>2</sub> ≥94%
Already had salbutamol via spacer — needs escalation to nebuliser + ipratropium
IV MgSO<sub>4</sub> is indicated if poor response AFTER first-line severe treatment — not yet
CXR not immediate priority — treat first, investigate if deteriorates
IV aminophylline is last resort — multiple steps before this
<b>IV MgSO<sub>4</sub> (40mg/kg, max 2g)</b> is the key escalation after salbutamol + ipratropium in SEVERE asthma not responding to first-line treatment. Common exam question!
<b>SpO<sub>2</sub> <92%</b> = SEVERE
<b>SpO<sub>2</sub> <92% + silent chest + exhaustion</b> = LIFE-THREATENING → call senior NOW
Exam Pearls
Asthma: Key Facts
Under-5s diagnosed clinically — no spirometry
Salbutamol response (≥12% FEV1 increase) supports diagnosis
SpO2 <92% = <b>SEVERE</b> <span style="color:#CBD5E1; margin:0 8px;">|</span> Silent chest + exhaustion = <b>LIFE-THREATENING</b>
Step up ONLY after checking inhaler technique & adherence
Ipratropium bromide: ONLY add in <b>SEVERE/LIFE-THREATENING</b> — not mild/moderate
<b>IV MgSO4</b> = key escalation after failed back-to-back nebs in severe asthma
Life-threatening features:
<span style="background: rgba(220,38,38,0.1); padding: 5px 14px; border-radius: 6px;">Silent chest</span> <span style="color:#FCA5A5; font-size: 20px;">•</span> <span style="background: rgba(220,38,38,0.1); padding: 5px 14px; border-radius: 6px;">Cyanosis</span> <span style="color:#FCA5A5; font-size: 20px;">•</span> <span style="background: rgba(220,38,38,0.1); padding: 5px 14px; border-radius: 6px;">Poor respiratory effort</span> <span style="color:#FCA5A5; font-size: 20px;">•</span> <span style="background: rgba(220,38,38,0.1); padding: 5px 14px; border-radius: 6px;">Exhaustion</span> <span style="color:#FCA5A5; font-size: 20px;">•</span> <span style="background: rgba(220,38,38,0.1); padding: 5px 14px; border-radius: 6px;">Altered GCS</span> <span style="color:#FCA5A5; font-size: 20px;">•</span> <span style="background: rgba(220,38,38,0.1); padding: 5px 14px; border-radius: 6px;">Bradycardia/Bradypnoea</span>
02
Section 2
BRONCHIOLITIS
RSV | Diagnosis | Admission Criteria | Supportive Management
Epidemiology
RSV Pathophysiology
NICE Admission Criteria
NICE Discharge Criteria
Supportive Management
Common Exam Traps
<span style="color: #006670; font-weight: 700;">UKMLA</span> Curriculum Aligned | BTS/SIGN | NICE | RCPCH
Bronchiolitis: Presentation & Diagnosis
Key Facts
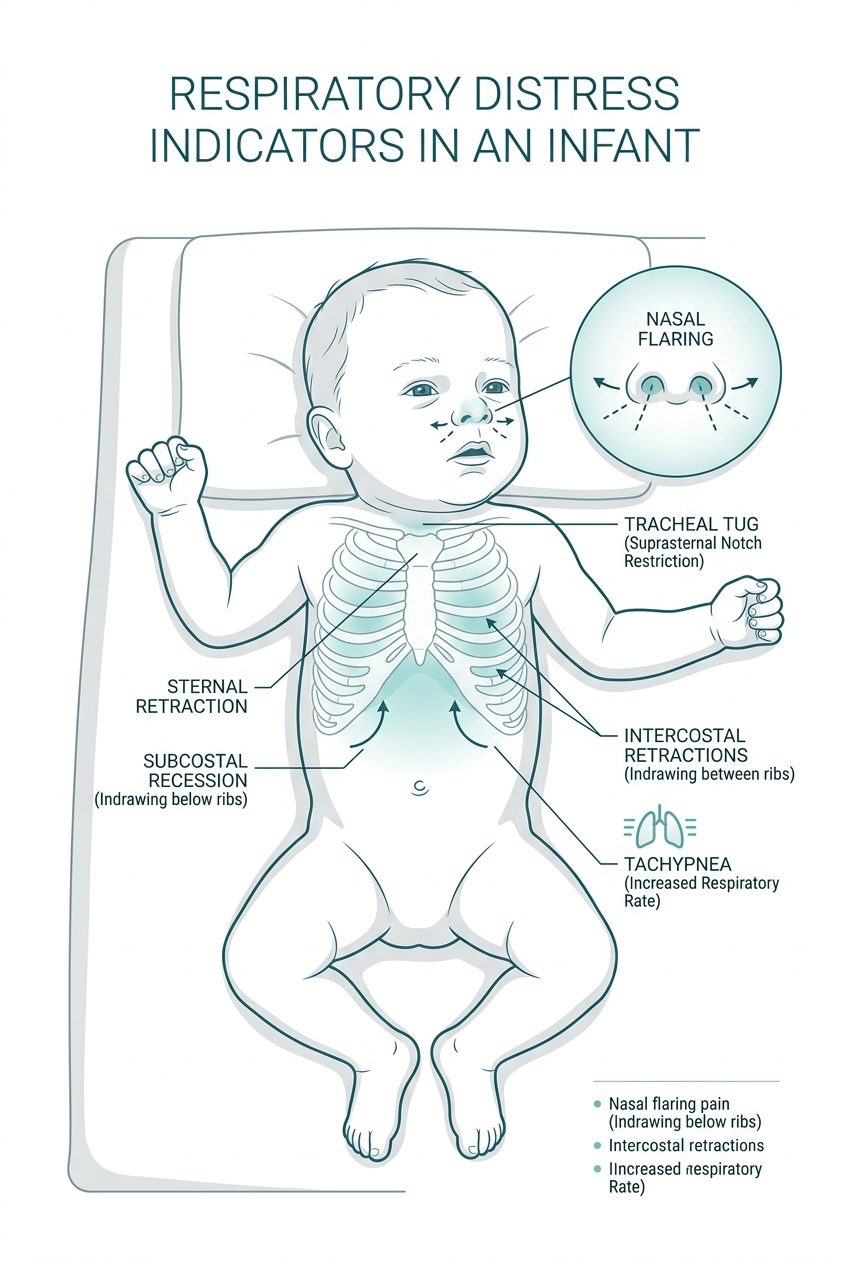
Clinical Features
Red Flags for Severe Disease
<strong>Diagnosis is CLINICAL.</strong> No routine bloods, CXR or viral swabs needed in typical presentation.
NICE Bronchiolitis: Management Flowchart
Infant with bronchiolitis — Assess severity
📋 SBA QUESTION 3
A 3-month-old infant (born at 34 weeks gestation) is brought to the ED in December with a 2-day history of cough, runny nose, and poor feeding.
On examination: RR 62/min, SpO2 91% on air, intercostal recession, widespread wheeze and crackles. Temperature 37.8°C. He is taking approximately 40% of his normal feeds.
Which of the following is the MOST appropriate management?
Administer nebulised salbutamol and reassess in 1 hour
Start oral prednisolone 1mg/kg and discharge with safety netting
Admit, apply supplemental oxygen, and consider nasogastric feeds
Start amoxicillin 125mg TDS for 5 days
Discharge home with intranasal saline drops and safety netting advice
Think: What makes this child HIGH RISK? What does NICE say about O2 threshold?
Answer on next slide
ANSWER: C
Correct Answer: C — Admit, supplemental oxygen, consider NG feeds
<b>SpO2 91%</b> < NICE threshold of 92% → supplemental O2 required
<b>Feeds 40% of normal</b> → below 50% threshold → NG feeds indicated
<b>Premature (34 weeks gestation)</b> → HIGH RISK group → automatic consideration for admission
Combined: SpO2 <92% + poor feeding + prematurity = <b>clear admission criteria</b>
Apnoeas in bronchiolitis = immediate escalation → PICU/HDU input
<b>Salbutamol NOT indicated</b> — no RCT evidence, NICE recommends against routine use
<b>Steroids NOT indicated</b> — no evidence of benefit in bronchiolitis
<b>Antibiotics</b> — viral illness, no indication unless proven secondary bacterial infection
<b>Unsafe to discharge</b> — SpO2 <92%, poor feeding, premature = all admission criteria
SpO2 <92% = O2 threshold in bronchiolitis
Feeds <50% normal = NG tube indication
Prematurity <37 weeks = high-risk factor for severe disease
03
Section 3
PNEUMONIA & LRTI
Viral vs Bacterial | Investigations | NICE Antibiotics | Complications
Viral vs Bacterial
CXR Interpretation
Severity Assessment
PEWS
Antibiotic Choice
Complications
Viral vs Bacterial Pneumonia
Key Differences
CLINICAL COMPARISON
NICE:
Amoxicillin is first-line for uncomplicated bacterial pneumonia. Use clarithromycin if atypical (Mycoplasma) suspected. CXR NOT routinely required in uncomplicated cases.
Pneumonia: Assessment & Management
Mild
Manage at home
Oral amoxicillin 40mg/kg/day TDS 5 days
Safety net
Review 48hrs
Moderate
Consider admission
Oral/IV amoxicillin
O₂ if SpO₂ < 94%
IV fluids if needed
CXR
Severe
Admit immediately
IV amoxicillin + O₂
Blood cultures | FBC/CRP/U&E | CXR
Consider co-amoxiclav or ceftriaxone if no improvement
Antibiotic Guide
Uncomplicated Bacterial
Amoxicillin 40mg/kg/day (oral, 5 days)
Atypical (Mycoplasma)
Clarithromycin / Azithromycin
Penicillin Allergy
Clarithromycin
Staphylococcal
Flucloxacillin ± Rifampicin
MRSA
IV Vancomycin
Complications
Parapneumonic effusion
Empyema
Lung abscess
Septicaemia
Clinical Pearls
CXR shows LOBAR CONSOLIDATION in bacterial pneumonia.
Bilateral perihilar changes = viral.
Round pneumonia = classic for Strep pneumoniae in young children.
📋 SBA QUESTION 4
A 5-year-old boy is brought to his GP with a 3-day history of high fever (39.5°C), rigors, and productive cough. He appears unwell with RR 38/min, SpO2 95% on air, dull percussion and bronchial breathing in the right lower zone.
He has no known drug allergies.
What is the MOST appropriate antibiotic treatment?
Co-amoxiclav 400/57mg oral suspension
Amoxicillin 250mg TDS oral for 5 days
Clarithromycin 125mg BD oral for 5 days
Cefalexin 125mg QDS oral for 7 days
Doxycycline 100mg BD oral for 5 days
Think: What type of pneumonia is this? What does NICE recommend as first-line?
Answer on next slide →
B — Amoxicillin 250mg TDS for 5 days
<b>High fever + rigors + productive cough + focal signs</b> = bacterial pneumonia (Strep pneumoniae most likely)
<b>NICE recommends amoxicillin</b> as first-line for uncomplicated community-acquired bacterial pneumonia in children
No penicillin allergy mentioned → amoxicillin appropriate
SpO2 95% and able to take oral medications → outpatient oral treatment appropriate
A) Co-amoxiclav
reserve for complicated/hospital-acquired pneumonia, not first-line
C) Clarithromycin
for atypical (Mycoplasma) or penicillin allergy, not first-line uncomplicated
D) Cefalexin
not standard recommendation for pneumonia
E) Doxycycline
<b>NOT used in children <12 years</b> (teeth staining)
Amoxicillin = NICE first-line for uncomplicated bacterial CAP
Clarithromycin = atypical / penicillin allergy
Doxycycline contraindicated <12 years
CXR NOT required for uncomplicated cases
"Mycoplasma pneumoniae: school-age children, insidious onset, 'walking pneumonia', bilateral infiltrates on CXR, treat with macrolide."
04
SECTION 4
CROUP vs EPIGLOTTITIS
Diagnosis | Emergency Airway Management | When to Call for Help
Westley Croup Score
Dexamethasone
Nebulised Adrenaline
Epiglottitis Red Flags
ENT Involvement
Airway Emergency
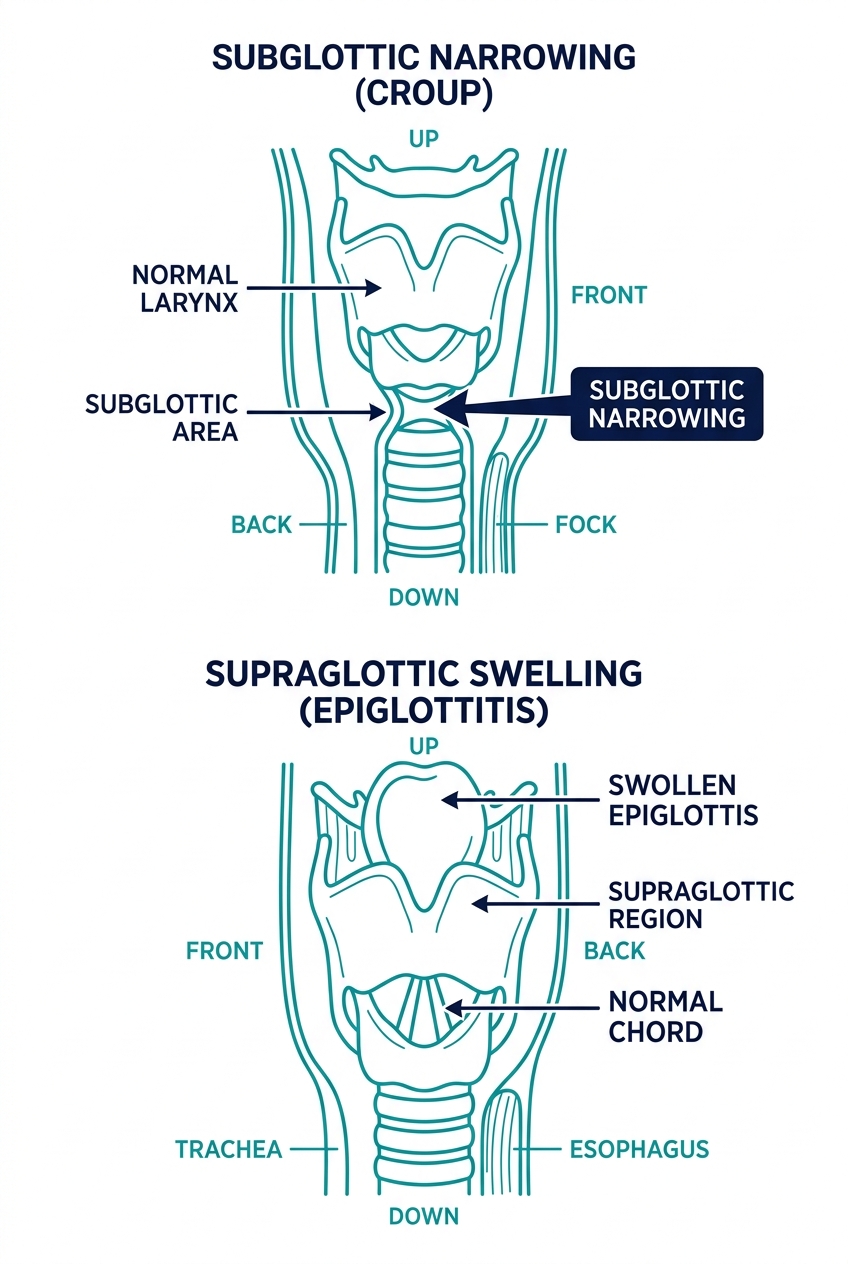
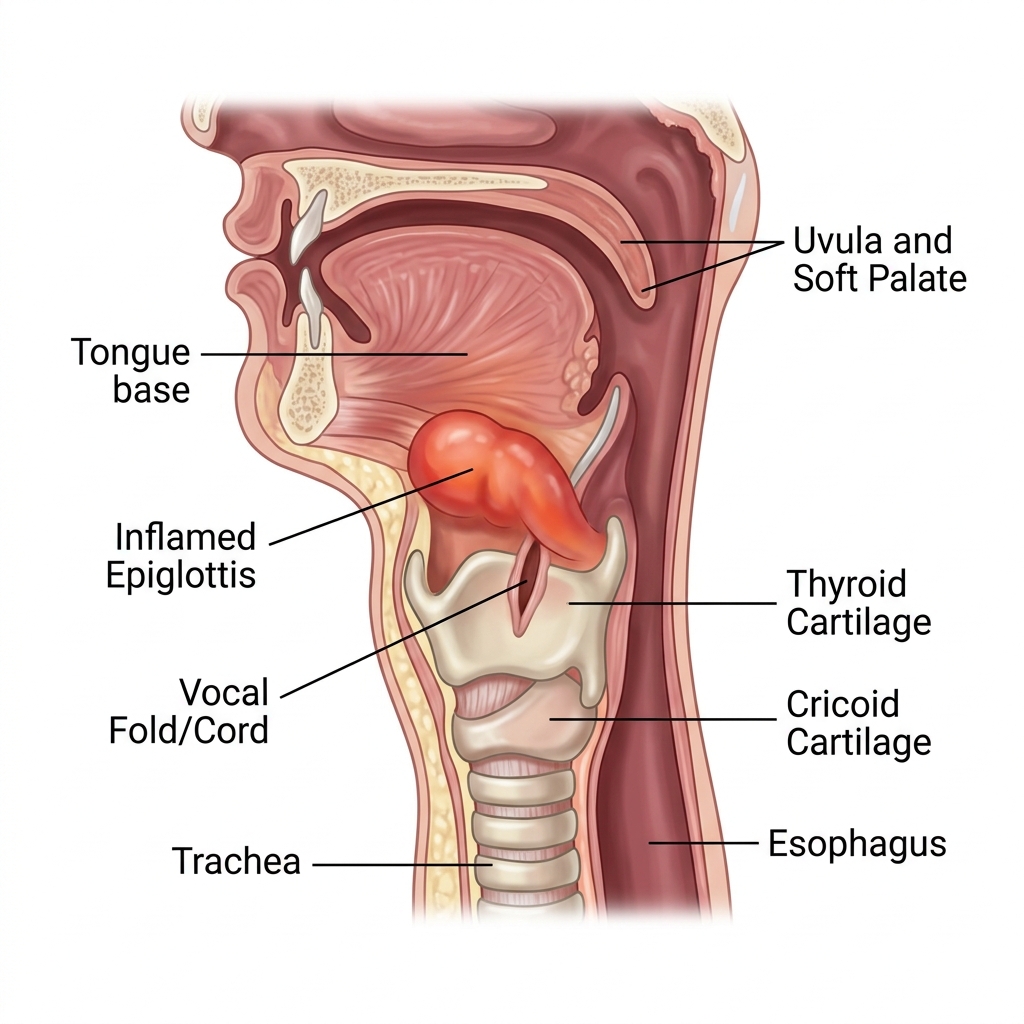
Croup vs Epiglottitis: Key Differentiating Features
CRITICAL WARNING
DO NOT examine the throat in suspected epiglottitis — may precipitate complete airway obstruction. Keep child calm. Senior help IMMEDIATELY.
Croup: Assessment & Management
Westley Croup Score
Score 0–2: MILD
Score 3–7: MODERATE
Score 8+: SEVERE
Features Scored
Level of consciousness
Cyanosis
Stridor
Air entry
Retractions
Management by Severity
MILD
Stay calm, reassure child
Oral dexamethasone 0.15mg/kg single dose
Discharge home
Review if worsens
MODERATE
Oral/IM dexamethasone
Humidified O2 if SpO2 <94%
Observe 4 hours
Discharge if improving
SEVERE
Nebulised adrenaline 5ml of 1:1000
O2
Dexamethasone
Admit
Anaesthetics aware
Key Drug Info
Dexamethasone
0.15mg/kg single dose oral
Reduces severity & duration
Works within 30 mins
Evidence-based
Neb Adrenaline
5ml 1:1000 nebulised
Short acting (2–3 hrs) — can rebound
Must admit after use
Bridge to dexamethasone
<strong>Dexamethasone single dose</strong> is effective even in mild croup. Onset 30 mins. <strong>Adrenaline = TEMPORARY</strong> — always combine with dexamethasone and admit.
📋 SBA QUESTION 5
A 3-year-old boy is brought to the ED by ambulance. He developed a severe sore throat 4 hours ago and is now sitting upright leaning forward, drooling saliva, and appears extremely distressed and toxic. His temperature is 39.8°C. He is making soft inspiratory noise. He has had all his routine immunisations.
What is the SINGLE MOST IMPORTANT immediate action?
Give nebulised adrenaline immediately
Administer oral dexamethasone 0.15mg/kg
Ask the child to open his mouth and inspect the throat with a tongue depressor
Call senior paediatric, anaesthetic, and ENT teams urgently — keep child calm
Arrange urgent lateral neck X-ray
What clinical features point to epiglottitis vs croup? What must you NOT do?
Answer on next slide →
<strong>Epiglottitis mnemonic: The 4 Ds</strong><br>Drooling, Dysphagia, Distress, Dysphonia (muffled voice)
Correct Answer: D — Call senior paediatric, anaesthetic, and ENT teams urgently — keep child calm
NEVER examine the throat in suspected epiglottitis. Keep the child calm. Any distress can precipitate complete obstruction. This is a theatre emergency.
📋 SBA QUESTION 6
Croup Management
An 18-month-old girl is brought to the ED at 2am with a 12-hour history of barking cough and inspiratory stridor.
She is mildly distressed, has mild subcostal recession, audible stridor at rest, SpO2 97%, and RR 32/min. She is alert and taking fluids well. Westley score = 4.
What is the MOST appropriate management?
Admit for IV antibiotics and close monitoring
Give nebulised adrenaline and discharge once improved
Give a single dose of oral dexamethasone 0.15mg/kg and observe for 4 hours
Arrange CT neck to identify the cause of stridor
Give humidified oxygen via tent and monitor overnight
THINK
Westley score 4 = what severity?<br>What is first-line treatment?
Answer on next slide →
✅ ANSWER: C
Correct Answer: C — Oral dexamethasone 0.15mg/kg single dose + observe 4 hours
<b>Classic croup:</b> barking cough, inspiratory stridor, 18-month-old, 2am presentation
<b>Westley Score 4</b> = MODERATE croup
<b>Stridor at rest</b> = indicates moderate severity
<b>First-line treatment</b> = oral dexamethasone 0.15mg/kg single dose
<b>Observe for 4 hours</b> post-treatment then discharge if improving
<b>SpO2 97%</b> — no need for supplemental oxygen
<b>IV antibiotics</b> — croup is viral (parainfluenza), not bacterial; antibiotics not indicated
<b>Nebulised adrenaline</b> — reserved for SEVERE croup (Westley ≥8) or imminent respiratory failure; must admit after use due to rebound
<b>CT neck</b> — not appropriate in emergency; clinical diagnosis
<b>Humidified oxygen tent</b> — evidence does NOT support; can upset child
"Dexamethasone 0.15mg/kg single oral dose — works in 30 minutes. Even mild croup benefits from a single dose. Nebulised budesonide = alternative if unable to swallow."
05
SECTION 5
CYSTIC FIBROSIS
Genetics | Screening | Diagnosis | Multisystem Management | CFTR Modulators
CFTR Genetics
Heel Prick Screening
Sweat Chloride Test
Respiratory Management
GI & Nutrition
CFTR Modulators
Respiratory Medicine
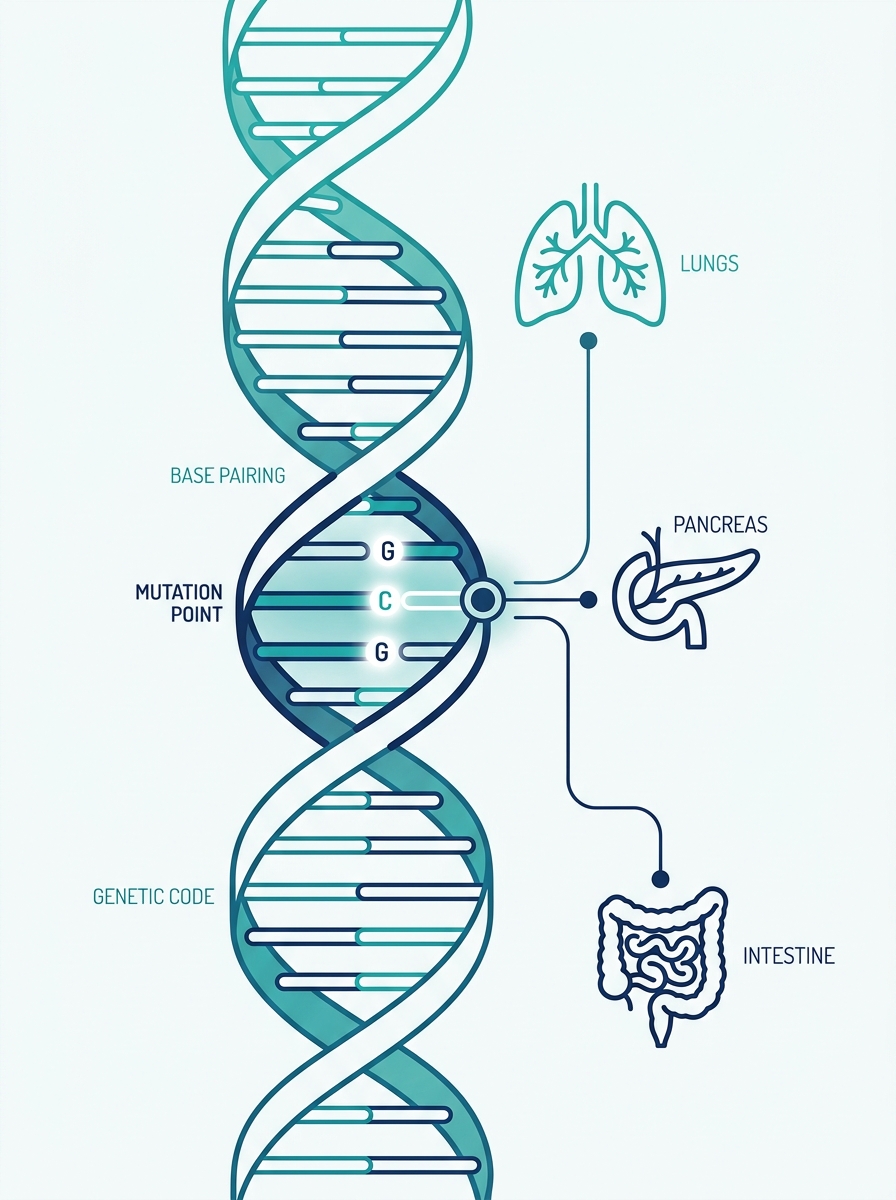
Cystic Fibrosis: Genetics & Diagnosis
Genetics
Screening
Diagnostic Tests
Most common = F508del. Sweat chloride ≥60 = diagnostic. CFTR = Cystic Fibrosis Transmembrane conductance Regulator.
Cystic Fibrosis
Multisystem Clinical Features
CF Management: MDT Approach
RESPIRATORY
Chest physiotherapy (twice daily)
Airway clearance (Active Cycle of Breathing)
<strong>DNase (dornase alfa)</strong> — reduces sputum viscosity
Hypertonic saline (inhaled)
Prophylactic azithromycin (Pseudomonas)
Tobramycin inhaled (Pseudomonas)
Annual influenza vaccine
NUTRITIONAL
High calorie, high fat diet
<strong>PERT</strong> — Creon with every meal
Fat-soluble vitamins: <strong>A, D, E, K</strong> supplementation
NG/gastrostomy feeding if needed
Dietitian input
CFTR MODULATORS
<strong>Ivacaftor</strong> (G551D mutation) — potentiator
<strong>Lumacaftor/ivacaftor</strong> (Orkambi) — F508del homozygous
<strong>Tezacaftor/ivacaftor</strong> — F508del
<strong>Elexacaftor/tezacaftor/ivacaftor</strong> (Kaftrio) — F508del — <span style="background-color: #FEF3C7; color: #B45309; border: 1px solid #F59E0B; padding: 2px 8px; border-radius: 6px; font-weight: 800; font-size: 16px; margin-left: 6px; vertical-align: middle;">GAME CHANGER</span>
Available on NHS — dramatically improves lung function
MDT & MONITORING
3-monthly clinic reviews
Annual lung function tests
Annual OGTT (screen CF-related diabetes)
Microbiology surveillance
Psychosocial support
Genetic counselling
Clinical Pearl
<strong>Kaftrio (elexacaftor/tezacaftor/ivacaftor)</strong> is eligible for <strong>~90%</strong> of CF patients with <strong>≥1 F508del allele</strong>.<br>Transformative — reduces hospitalisations by <strong>>60%</strong>.
SBA QUESTION 7
A 6-week-old boy is referred to the paediatric team because his newborn blood spot screening showed a raised immunoreactive trypsinogen (IRT) level. A sweat chloride test is performed, showing a result of 72 mmol/L. Genetic testing reveals he is homozygous for F508del.
Which of the following is the MOST appropriate initial dietary supplement he will require?
Iron and folic acid supplementation
Calcium and vitamin D supplementation
Fat-soluble vitamins A, D, E, and K
Medium-chain triglyceride (MCT) oil exclusively
Water-soluble B and C vitamins
Think
What is the most common nutritional deficiency in CF? Why?
Answer on next slide →
✅ ANSWER: C
Fat-soluble vitamins A, D, E, and K
Explanation
CF causes exocrine pancreatic insufficiency <strong style='color: #0D2C4E;'>→</strong> reduced secretion of lipase/protease
Without lipase <strong style='color: #0D2C4E;'>→</strong> fat malabsorption <strong style='color: #0D2C4E;'>→</strong> fat-soluble vitamins (A, D, E, K) are not absorbed
Leads to deficiencies of vitamins A (vision), D (bones), E (neuro), K (coagulation)
ALL CF patients with pancreatic insufficiency need routine fat-soluble vitamin supplementation
Water-soluble vitamins (B, C) are absorbed normally <strong style='color: #0D2C4E;'>→</strong> no routine supplementation needed
Why the others are wrong
<strong style='color: #0D2C4E; font-size: 24px;'>A) Iron/folate</strong><br><span style='margin-top: 6px; display: inline-block;'>Not the primary concern in CF.</span>
<strong style='color: #0D2C4E; font-size: 24px;'>B) Calcium/Vit D alone</strong><br><span style='margin-top: 6px; display: inline-block;'>Incomplete; all A, D, E, K needed.</span>
<strong style='color: #0D2C4E; font-size: 24px;'>D) MCT oil</strong><br><span style='margin-top: 6px; display: inline-block;'>Used adjunctly, not primary supplement.</span>
<strong style='color: #0D2C4E; font-size: 24px;'>E) Vit B & C</strong><br><span style='margin-top: 6px; display: inline-block;'>Absorbed normally in CF.</span>
💡 CLINICAL PEARL
CF nutrition = 3 things to remember:
Fat-soluble vitamins <strong style='color: #B45309;'>A, D, E, K</strong> supplementation
Pancreatic enzyme replacement (<strong style='color: #B45309;'>PERT/Creon</strong>) with every meal and snack
<strong style='color: #B45309;'>High-calorie, high-fat diet</strong> (120% normal requirement)
🚨 RED FLAG
Vitamin K deficiency in CF <strong style='color: #7F1D1D;'>→ coagulopathy →</strong> bruising, bleeding. <span style='background-color: #FECACA; padding: 2px 8px; border-radius: 4px;'>Check INR if unwell.</span>
📋 SBA QUESTION 8
Both parents of a 2-year-old girl have been found to be carriers of the CFTR F508del mutation. They ask about the probability that their next child will also have cystic fibrosis.
What is the probability that their next child will have cystic fibrosis?
1 in 2 (50%)
1 in 4 (25%)
1 in 8 (12.5%)
2 in 3 (67%)
3 in 4 (75%)
Think: What is the inheritance pattern of CF? Draw a Punnett square mentally.
Answer on next slide →
ANSWER: B — 1 in 4 (25%)
FINAL REVISION ROUND
RAPID-FIRE REVISION ROUND
15 UKMLA-Style SBA Questions <span style='color: #94A3B8; margin: 0 10px;'>|</span> Mixed Topics <span style='color: #94A3B8; margin: 0 10px;'>|</span> Single Best Answer
All Sections
Exam Difficulty
With Full Explanations
Asthma <span style='color: #CBD5E1; margin: 0 10px;'>|</span> Bronchiolitis <span style='color: #CBD5E1; margin: 0 10px;'>|</span> Pneumonia <span style='color: #CBD5E1; margin: 0 10px;'>|</span> Croup <span style='color: #CBD5E1; margin: 0 10px;'>|</span> Epiglottitis <span style='color: #CBD5E1; margin: 0 10px;'>|</span> Cystic Fibrosis
Try to answer each question before the answer is revealed
Rapid Fire: Questions 1–5
Q1
A 4-year-old with nocturnal wheeze and cough. Spirometry cannot be performed reliably. What is the MOST appropriate diagnostic approach?
<div style="display: flex; gap: 24px; flex-wrap: wrap; line-height: 1.4; align-items: center;"><div>A) FeNO</div><div>B) Peak flow monitoring</div><div style="color: #166534; font-weight: 800; background-color: #DCFCE7; padding: 2px 10px; border-radius: 6px;">C) Trial of salbutamol MDI + spacer</div><div>D) CT chest</div><div>E) Allergy testing</div></div>
C
Q2
A 2-month-old with 3-day cough, wheeze, SpO2 93%, feeds 60% normal. Born at term. What is the MOST appropriate management?
<div style="display: flex; gap: 24px; flex-wrap: wrap; line-height: 1.4; align-items: center;"><div>A) Discharge with safety netting</div><div style="color: #166534; font-weight: 800; background-color: #DCFCE7; padding: 2px 10px; border-radius: 6px;">B) Admit, O2, monitor feeds</div><div>C) Salbutamol nebs</div><div>D) Oral steroids</div><div>E) Antibiotics</div></div>
B
Q3
Which organism is responsible for the majority of croup cases?
<div style="display: flex; gap: 24px; flex-wrap: wrap; line-height: 1.4; align-items: center;"><div>A) Streptococcus pneumoniae</div><div>B) Haemophilus influenzae</div><div style="color: #166534; font-weight: 800; background-color: #DCFCE7; padding: 2px 10px; border-radius: 6px;">C) Parainfluenza virus</div><div>D) RSV</div><div>E) Rhinovirus</div></div>
C
Q4
A child has PEFR 40%, speaks in short sentences, SpO2 93%. What severity of asthma?
<div style="display: flex; gap: 24px; flex-wrap: wrap; line-height: 1.4; align-items: center;"><div>A) Mild</div><div style="color: #166534; font-weight: 800; background-color: #DCFCE7; padding: 2px 10px; border-radius: 6px;">B) Moderate</div><div>C) Severe</div><div>D) Life-threatening</div><div>E) Pre-attack</div></div>
B <span style="font-size: 15px; margin-left: 8px; font-weight: 700; opacity: 0.9;">(Moderate: 33-50%)</span>
Q5
Which antibiotic is first-line for uncomplicated CAP in a 6-year-old?
<div style="display: flex; gap: 24px; flex-wrap: wrap; line-height: 1.4; align-items: center;"><div>A) Co-amoxiclav</div><div>B) Clarithromycin</div><div style="color: #166534; font-weight: 800; background-color: #DCFCE7; padding: 2px 10px; border-radius: 6px;">C) Amoxicillin</div><div>D) Cefalexin</div><div>E) Doxycycline</div></div>
C
Rapid Fire: Questions 6–10
Recap Section
A child with epiglottitis is in ED. Which action is CONTRAINDICATED?
A) Calling anaesthetics
B) Applying high-flow O2
<span style="color: #006670; font-weight: 700;">C) Examining throat with tongue depressor</span>
D) Keeping child calm
E) Starting IV ceftriaxone
ANSWER: C
CF newborn screening: IRT is raised. What is the NEXT step?
A) Sweat chloride test immediately
<span style="color: #006670; font-weight: 700;">B) DNA mutation analysis</span>
C) CXR
D) Bronchoscopy
E) Discharge and review at 6 weeks
ANSWER: B
A 7-month-old admitted with bronchiolitis. SpO2 drops to 91%. What is the SpO2 threshold for supplemental O2 per NICE?
A) 90%
<span style="color: #006670; font-weight: 700;">B) 92%</span>
C) 94%
D) 96%
E) 98%
ANSWER: B
CXR shows steeple sign. Diagnosis?
A) Epiglottitis
B) Foreign body
<span style="color: #006670; font-weight: 700;">C) Croup</span>
D) Bacterial tracheitis
E) Retropharyngeal abscess
ANSWER: C
A CF patient aged 12 is homozygous F508del. Which CFTR modulator is most likely prescribed?
A) Ivacaftor alone
B) Lumacaftor/ivacaftor
<span style="color: #006670; font-weight: 700;">C) Elexacaftor/tezacaftor/ivacaftor (Kaftrio)</span>
D) Tezacaftor alone
E) No modulator available
ANSWER: C
⚡ Rapid Fire: Questions 11–15
Life-threatening asthma features include all EXCEPT:
A) Silent chest • B) SpO₂ <92% • C) PEFR >50% • D) Cyanosis • E) Exhaustion
C
(PEFR >50% is MILD)
A 5-year-old with 'walking pneumonia', dry cough, bilateral infiltrates on CXR, normal WBC. Likely organism?
A) S. pneumoniae • B) S. aureus • C) Mycoplasma pneumoniae • D) RSV • E) H. influenzae
C
(Mycoplasma pneumoniae)
What is the gold standard diagnostic test for Cystic Fibrosis?
A) Genetic mutation • B) CXR • C) Nasal potential difference • D) Sweat chloride test • E) IRT
D
(Sweat chloride test)
Nebulised adrenaline is given for severe croup. After improvement, what MUST happen?
A) Discharge immediately • B) Admit for observation • C) Repeat after 30 mins • D) Give oral pred & discharge • E) Arrange ENT review
B
(Admit due to rebound risk)
A 6-week-old (premature, 33 weeks) presents with bronchiolitis, SpO₂ 95%, feeds 80% normal, mild recession. MOST appropriate management?
A) Discharge • B) Admit for observation (high-risk) • C) Salbutamol • D) Start steroids • E) CXR & blood cultures
B
(Premature <37wks = high risk)
⚡ Rapid Fire: Key Explanations
Trickiest Q&A Points from Q1-15
Q1
Asthma Diagnosis
<b style="color: #0D2C4E; font-weight: 700;">Under-5s = clinical diagnosis only.</b> Trial of salbutamol MDI + spacer is the practical diagnostic tool. Spirometry unreliable.
Q5
Pneumonia Antibiotics
<b style="color: #0D2C4E; font-weight: 700;">Amoxicillin = NICE first-line for CAP.</b> Doxycycline contraindicated <12 years (teeth staining).
Q8
Bronchiolitis O₂ Goal
<b style="color: #006670; font-weight: 700;">NICE bronchiolitis O₂ threshold = SpO₂ <92%.</b> Different from asthma threshold (94%).
Q11
Asthma Severity
<b style="color: #006670; font-weight: 700;">PEFR >50% = MILD asthma.</b> Life-threatening = PEFR <33% + silent chest + SpO₂ <92% + exhaustion.
Q14
Croup Management
<b style="color: #0D2C4E; font-weight: 700;">Nebulised adrenaline is SHORT-ACTING (2-3 hrs).</b> After improvement, child MUST be admitted — rebound stridor can occur. Always combine with dexamethasone.
Q15
Bronchiolitis Admission
<b style="color: #0D2C4E; font-weight: 700;">Prematurity <37 weeks</b> = high-risk factor for severe bronchiolitis → admit for observation even if SpO₂ satisfactory.
What the UKMLA Wants You to Know
Core Knowledge Map — Paediatric Respiratory & ENT
ASTHMA
Diagnose using spirometry (>5yrs) or clinical/salbutamol trial (<5yrs) <span style="color: #CBD5E1; margin: 0 12px; font-weight: 300;">|</span> BTS/SIGN stepwise management <span style="color: #CBD5E1; margin: 0 12px; font-weight: 300;">|</span> Severity classification <span style="color: #CBD5E1; margin: 0 12px; font-weight: 300;">|</span> IV MgSO<sub style="font-size:16px">4</sub> in severe asthma
BRONCHIOLITIS
Clinical diagnosis (no bloods/CXR routinely) <span style="color: #CBD5E1; margin: 0 12px; font-weight: 300;">|</span> NICE admission criteria <span style="color: #CBD5E1; margin: 0 12px; font-weight: 300;">|</span> Supportive care <strong style="color: #064E3B; font-weight: 800;">only</strong> <span style="color: #CBD5E1; margin: 0 12px; font-weight: 300;">|</span> No salbutamol/steroids/antibiotics
PNEUMONIA
Viral vs bacterial features <span style="color: #CBD5E1; margin: 0 12px; font-weight: 300;">|</span> <strong>Amoxicillin</strong> first-line <span style="color: #CBD5E1; margin: 0 12px; font-weight: 300;">|</span> <strong>Clarithromycin</strong> = atypical/penicillin allergy <span style="color: #CBD5E1; margin: 0 12px; font-weight: 300;">|</span> CXR not routine
Croup vs Epiglottitis
Barking cough + stridor = <strong>croup</strong> <span style="color: #EF4444; font-weight: 900; margin: 0 6px;">→</span> dexamethasone <span style="color: #CBD5E1; margin: 0 12px; font-weight: 300;">|</span> Drooling + tripod + toxic = <strong>epiglottitis</strong> <span style="color: #EF4444; font-weight: 900; margin: 0 6px;">→</span> DO NOT examine throat <span style="color: #EF4444; font-weight: 900; margin: 0 6px;">→</span> emergency team
CYSTIC FIBROSIS
Autosomal recessive, <strong>F508del</strong> most common <span style="color: #CBD5E1; margin: 0 12px; font-weight: 300;">|</span> Sweat chloride ≥60 = diagnostic <span style="color: #CBD5E1; margin: 0 12px; font-weight: 300;">|</span> MDT management <span style="color: #CBD5E1; margin: 0 12px; font-weight: 300;">|</span> CFTR modulators (Kaftrio)
UKMLA Content Map:
Covered — Respiratory disorders in children <span style="color: rgba(255,255,255,0.4); margin: 0 12px;">|</span> Emergency paediatrics <span style="color: rgba(255,255,255,0.4); margin: 0 12px;">|</span> Genetic conditions
Top 10 Exam Pearls
Under-5s: Asthma diagnosed <strong style="color: #006670; font-weight: 800;">CLINICALLY</strong> — no spirometry
SpO2 <92% = <strong style="color: #006670; font-weight: 800;">SEVERE</strong> asthma | <92% + silent chest + exhaustion = <strong style="color: #006670; font-weight: 800;">LIFE-THREATENING</strong>
<strong style="color: #006670; font-weight: 800;">IV MgSO4</strong> (40mg/kg) = escalation after salbutamol + ipratropium failure in severe asthma
Bronchiolitis = <strong style="color: #006670; font-weight: 800;">SUPPORTIVE CARE ONLY</strong>. No salbutamol, no steroids, no antibiotics
<strong style="color: #006670; font-weight: 800;">SpO2 <92%</strong> = O2 threshold in bronchiolitis (NICE)
<strong style="color: #006670; font-weight: 800;">Amoxicillin</strong> = first-line for uncomplicated bacterial CAP. Doxycycline contraindicated <12 years
Epiglottitis = <strong style="color: #EF4444; font-weight: 800;">DO NOT</strong> examine throat. Keep calm. Emergency: paeds + anaesthetics + ENT
The 4 Ds of epiglottitis: <strong style="color: #006670; font-weight: 800;">Drooling, Dysphagia, Distress, Dysphonia</strong>
Croup: <strong style="color: #006670; font-weight: 800;">steeple sign</strong> on CXR | Epiglottitis: <strong style="color: #006670; font-weight: 800;">thumbprint sign</strong>
CF: <strong style="color: #006670; font-weight: 800;">F508del</strong> most common | Sweat chloride <strong style="color: #006670; font-weight: 800;">≥60</strong> = diagnostic | Kaftrio = CFTR modulator
⚠️ Common Exam Traps — Don't Fall For These!
TRAP 1
Giving salbutamol for bronchiolitis
<b>No evidence.</b> Answer = supportive care. <span style="font-size: 16px; opacity: 0.85; margin-left: 6px;">(Commonest bronchiolitis trap)</span>
TRAP 2
Starting ICS as Step 1 in asthma for all children
<b>SABA first</b> for mild intermittent. ICS = Step 2 only.
TRAP 3
Examining the throat in epiglottitis
<b>FATAL.</b> Can cause complete airway obstruction.
TRAP 4
Using doxycycline in a 10-year-old with pneumonia
<b>Contraindicated <12 years.</b> Use clarithromycin.
TRAP 5
Giving nebulised adrenaline and discharging croup
<b>Adrenaline is SHORT-ACTING</b> (rebound). Must admit.
TRAP 6
Thinking CF is diagnosed by genetic testing alone
<b>Sweat chloride ≥60</b> is the GOLD STANDARD. Genetics is confirmatory.
TRAP 7
Ordering routine CXR for mild bronchiolitis or uncomplicated CAP
<b>Not indicated</b> in uncomplicated cases (NICE).
TRAP 8
Prescribing antibiotics for croup
<b>Viral — parainfluenza.</b> Steroids not antibiotics.
Key Drug Doses — Paediatric Respiratory
Always check BNFc for precise weight-based dosing in clinical practice.
Session 1 Complete!
Paediatric Respiratory & ENT Emergencies
What we covered today:
<strong>Asthma</strong> — diagnosis, stepwise management, acute exacerbations
<strong>Bronchiolitis</strong> — RSV, NICE criteria, supportive care only
<strong>Pneumonia</strong> — viral vs bacterial, antibiotic choice
<strong>Croup vs Epiglottitis</strong> — recognition, emergency management
<strong>Cystic Fibrosis</strong> — genetics, screening, MDT management
Further Resources:
📚 Passmedicine
📱 Quesmed
📖 BNFc
🌐 NICE Guidelines
Questions? Good luck with your UKMLA!
- paediatrics
- asthma-management
- bronchiolitis
- pneumonia
- ukmla
- medical-education
- cystic-fibrosis