



Paediatric Life-Threats: Emergency Clinical CPD Guide
A JRCALC-aligned clinical guide for ambulance crews on managing paediatric respiratory failure, sepsis, and cardiac arrest in emergency pre-hospital care.
Paediatric Life-Threats: Small Margins, Massive Gravity
A JRCALC-aligned approach to Respiratory Failure, Sepsis, and Arrest
UK Ambulance Service Clinical CPD | 2026
Objectives & Ground Rules
<ul><li>Re-frame paediatric assessment using 'Structural Confidence' vs 'Panic'.</li><li>Standardise recognition of the 'Pre-Arrest' state (Resp/Circ).</li><li>Solidify JRCALC-aligned escalation pathways.</li></ul>
<ul><li><strong>NO MATHS IN HEADS:</strong> Use the App, JRCALC Page, or Broselow Tape.</li><li><strong>NO GUESSING:</strong> 'I think it's 5ml' is a forbidden phrase.</li><li><strong>STOP POINTS:</strong> We will identify moments to pause and check.</li></ul>
Human Factors in Paeds: Controlling the Chaos
<ul><li><strong>Designate a Lead:</strong> Even if only two crew members. One thinks, one does.</li><li><strong>Closed-Loop Comms:</strong> 'Preparing 100mcg Adrenaline' -> 'I heard 100mcg Adrenaline'.</li><li><strong>Cognitive Offloading:</strong> Use the JRCALC App for calculations. Don't rely on memory.</li><li><strong>The 10-for-10 Principle:</strong> Take 10 seconds to plan the next 10 minutes.</li></ul>
Assessment: The Paediatric A-E Approach
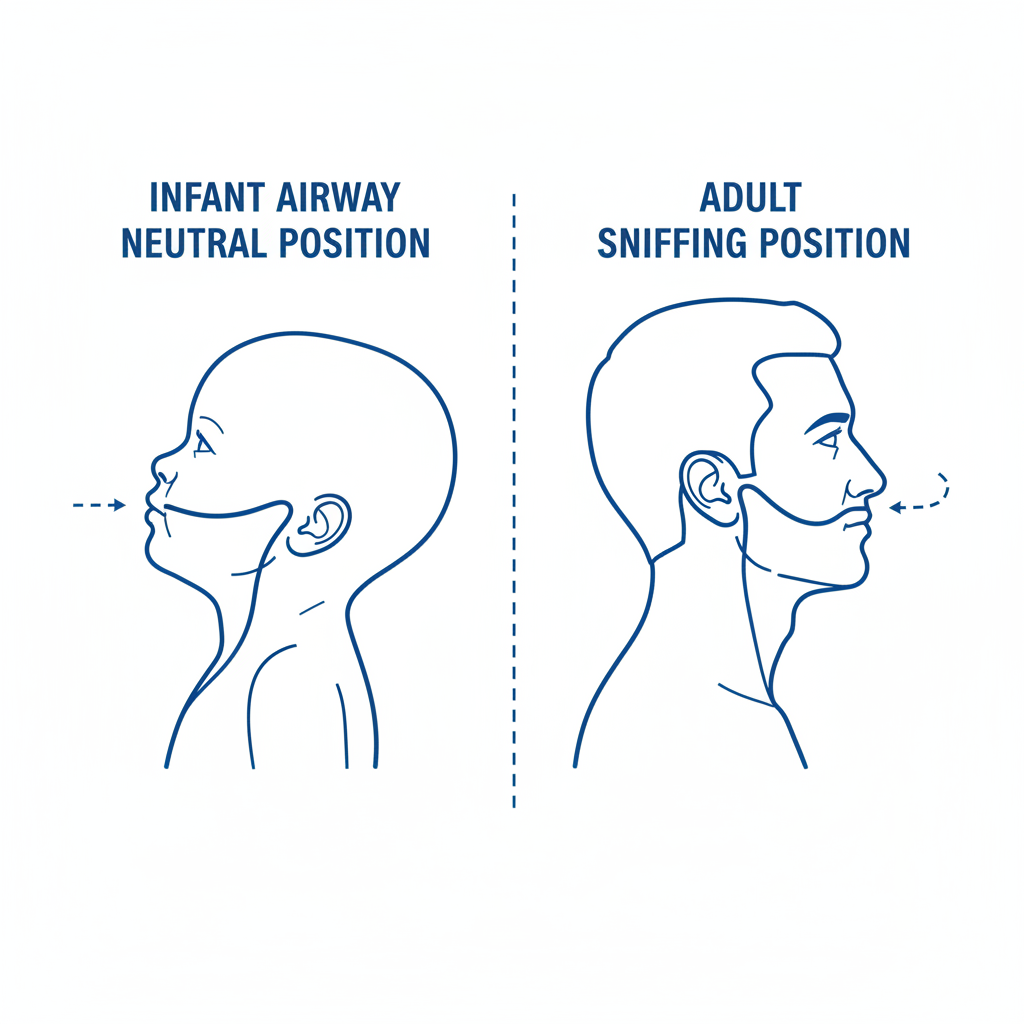
<h3>AIRWAY</h3><p>Clear? Stridor? Silent?<br>Neutral position (Infant) vs Sniffing (Child)</p>
<h3>BREATHING</h3><p>Effort vs Efficacy. Recession? Grunting?<br>Rate (Low is worse than High).</p>
<h3>CIRCULATION</h3><p>Rate. Rhythm. Vol. <br>Mottling (Red Flag)? CRT > 2s?</p>
<h3>DISABILITY</h3><p>AVPU. Glucose (Don't forget!).<br>Posterior Fontanelle tone.</p>
<h3>EXPOSURE</h3><p>Rashes (Glass Test). Trauma.<br>Temperature management.</p>
Airway: Anatomy & Basic Maneuvers
<ul><li><strong>Infants (< 1yr):</strong> Large occiput flexes head. Use 'Neutral Position'. Do NOT over-extend.</li><li><strong>Children (> 1yr):</strong> 'Sniffing the morning air' position.</li><li><strong>Adjuncts:</strong> Measure carefully (Corner of mouth to angle of jaw for OPA).</li><li><strong>Suction:</strong> Only under direct vision. Risk of vagal bradycardia or trauma.</li></ul>
STOP POINT: If Epiglottitis is suspected (drooling, tripod), DO NOT examine the airway. Keep calm, keep upright, transport immediately.
Breathing: The Decompensation Slope
<h3>1. Work of Breathing (WOB)</h3><p>Recession (Sub-costal/Inter-costal), Rate Increase, Nasal Flaring, Tracheal Tug.</p><h3>2. Exhaustion</h3><p>Head bobbing, 'See-saw' breathing, altered mental state (agitation -> drowsy).</p><h3>3. The Cliff Edge</h3><p><em>Silent Chest</em>, Bradycardia, Cyanosis. This is Pre-Arrest.</p>
Algorithm: Respiratory Failure Escalation
<strong>1. POSITION & O2</strong><br>Upright/Comfortable.<br>Oxygen 15L NRB if SpO2 < 94% or Shock.
<strong>2. TREAT CAUSE</strong><br>Nebs (Salbutamol/Atrovent/Adrenaline) per JRCALC.<br>Anaphylaxis? IM Adrenaline.
<strong>3. VENTILATE</strong><br>If exhaustion/apnoea/SpO2 falling:<br>BVM with O2. Add PEEP if protocol allows.
<strong>4. ADVANCED</strong><br>Consider I-Gel/LMA if BVM fails.<br>Pre-Alert for RSI/Critical Care.
Differentiation: Wheeze vs Croup vs Bronch
<h3>ASTHMA / WHEEZE</h3><p><strong>Cues:</strong> Expiratory wheeze, PMHx asthma, eczema.</p><p><strong>Rx:</strong> Salbutamol, Ipratropium, Hydrocortisone (Per JRCALC).</p>
<h3>CROUP</h3><p><strong>Cues:</strong> Barking cough, Stridor (Upper A/W), worse at night.</p><p><strong>Rx:</strong> Dexamethasone (PO/IV), Neb Adrenaline if severe (Per JRCALC).</p>
<h3>BRONCHIOLITIS</h3><p><strong>Cues:</strong> Infants (<2yr), wet cough, crackles, feeding difficulty.</p><p><strong>Rx:</strong> Supportive. Suction if blocked. O2 if hypoxic. NO Steroids/Nebs routinely.</p>
Sepsis: Recognition & The 'Paediatric 6'
<ul><li><strong>Rash:</strong> Non-blanching (late sign).</li><li><strong>Skin:</strong> Mottled / Ashen / Cyanosed.</li><li><strong>CRT:</strong> > 3 Seconds.</li><li><strong>HR:</strong> Significant Tachycardia OR Bradycardia (Ominous).</li><li><strong>RR:</strong> Tachypnoea / Grunting.</li><li><strong>Mentation:</strong> Lethargic / Unresponsive / Weak cry.</li></ul>
Parental Concern: 'They just aren't themselves' is a valid red flag.
Sepsis Action: The Golden Hour
<h3>1. OXYGEN</h3><p>High flow to maintain SpO2 >94%. Tissue perfusion is key.</p><h3>2. ACCESS</h3><p>IV preferred. If 2x failed attempts or critical → <strong>IO Access</strong> (Tibial/Humeral).</p>
<h3>3. FLUIDS</h3><p>Administer Bolus [volume per JRCALC/Kg]. Reassess lungs/liver after each bolus. Stop if rales/hepatomegaly.</p><h3>4. THERAPY</h3><p>Glucose (if low). Antibiotics (if PGD allows). Pre-alert 'Sepsis Six'.</p>
FLUID SAFETY: Rapid fluid boluses can cause heart failure in septic kids. 10-20ml/kg aliquots. CHECK JRCALC.
Medication Safety: Stop Points
<ul><li><strong>Two-Person Check:</strong> Clinician 1 reads JRCALC. Clinician 2 draws up. Swap and verify.</li><li><strong>Dilution Traps:</strong> E.g., Adrenaline 1:1,000 vs 1:10,000. Glucose concentrations.</li><li><strong>Weight:</strong> Estimated? Measured? Stated? (Document which one).</li><li><strong>Volume vs Dose:</strong> Confirm 'We are giving X mg, which is Y ml'.</li></ul>
Paediatric Cardiac Arrest: It's Different
<h3>Hypoxia is the Killer</h3><p>Unlike adults (often VF/VT primary), kids usually arrest due to progressive hypoxia and acidosis.</p><h3>Ventilation is Priority</h3><p>Focus on early oxygenation and ventilation breaths.</p><h3>Ratio: 15:2</h3><p>Use 15 compressions to 2 breaths for all paediatrics (unless newborn 3:1).</p>
Algorithm: Paediatric Advanced Life Support
<strong>CPR 15:2</strong><br>Rate 100-120.<br>Depth 1/3 Chest AP.<br>Minimize interruptions.
<strong>AIRWAY / O2</strong><br>100% O2.<br>BVM with adjuncts.<br>i-Gel/Tube if skilled.
<strong>ACCESS / DRUGS</strong><br>IO is first line if IV fails.<br>Adrenaline 1:10,000 [Dose/Kg].<br>Amiodarone if Shockable.
<strong>RHYTHM CHECK</strong><br>Shockable (VF/VT): 4 J/kg.<br>Non-Shockable (PEA/Asstole).
Conveyance & Escalation
<h3>Consider HEMS / Critical Care If:</h3><ul><li>RSI required (GCS < 8).</li><li>Ongoing seizure > 20 mins.</li><li>Post-ROSC care needed.</li><li>Logistical difficulty (Remote/Traffic).</li></ul>
<h3>ATMIST Pre-Alert</h3><ul><li><strong>A</strong>ge/Sex.</li><li><strong>T</strong>ime of onset.</li><li><strong>M</strong>echanism/Medical issue.</li><li><strong>I</strong>njuries/Insults found.</li><li><strong>S</strong>igns (Obs, GCS).</li><li><strong>T</strong>reatment given & ETA.</li></ul>
Case 1: The 'Wheezy' Toddler
<strong>SCENE:</strong> 2yo Male. 'Bad chest' for 2 days. Now lethargic.<br><strong>OBS:</strong> HR 180, RR 55, SpO2 88% (Air). Skin pale.<br><strong>AUSCULTATION:</strong> Very quiet chest. No obvious wheeze heard.
Decision Point: Is this asthma? Bronchiolitis? <br>Why is the chest quiet?
<strong>ANSWER:</strong> Silent Chest = Life Threatening Asthma/Bronchospasm.<br>Low air movement mimics 'clear' lungs. <br><strong>ACTION:</strong> High flow O2. Nebulised Adrenaline/Salbutamol driven by O2. Prepare BVM.
Case 2: The 'Sleepy' Infant
<strong>SCENE:</strong> 6mo Female. Fever. Vomiting x3. 'Hard to wake'.<br><strong>OBS:</strong> HR 190, RR 60, Temp 39.5C. Mottled legs.<br><strong>CRT:</strong> 4 seconds central.
Stop Point: Does this child need fluids? How much? How do we calculate?
<strong>ANSWER:</strong> Septic Shock. needs Fluid Resus.<br><strong>ACTION:</strong> 1. O2. 2. IV/IO Access. 3. Bolus 10-20ml/kg [per JRCALC]. 4. Glucose check.<br><strong>PITFALL:</strong> Delaying transport for IV attempts on scene. Do it en-route or use IO.
Summary & Takeaways
<h3>Breathing</h3><ul><li>Silence is deadly.</li><li>Treat hypoxia aggressively.</li><li>Nebs require flow.</li></ul>
<h3>Sepsis</h3><ul><li>Fluids for shock (check JRCALC).</li><li>IO is your friend.</li><li>Glucose is vital.</li></ul>
<h3>Arrest</h3><ul><li>15:2 Ratio.</li><li>Airway/Oxygen focus.</li><li>Use apps/guides for doses.</li></ul>
POST-JOB: Hot Debrief. Note safeguarding. Check your own welfare.
- paramedic-cpd
- paediatric-emergency
- jrcalc
- sepsis-recognition
- cardiac-arrest
- ambulance-service
- clinical-skills