


Managing Refractory Diarrhea in Metastatic Breast Cancer
A clinical review of diagnostic challenges for refractory diarrhea following chemotherapy and immunotherapy, focusing on C. diff, CMV, and IO-colitis.
Refractory Diarrhea in Metastatic Breast Cancer
Case Presentation: Diagnostic Dilemmas Post-Chemotherapy & Immunotherapy
Presented for Oncology Ward Review
Patient Profile & Admission
• Middle-aged female • Diagnosis: Metastatic Breast Cancer
• Recent Chemotherapy (Day 10 post-cycle) • Current Immunotherapy: Pembrolizumab
• Presented with: Nausea, vomiting, abdominal pain • Chief Complaint: Non-bloody loose stools
Initial Clinical Assessment
• Tachycardia on arrival • Other observations stable • ECG: Fast Atrial Fibrillation (AF)
• CRP > 400 mg/L (Severe Inflammation) • Hypokalemia (Low K+) • Hypomagnesemia (Low Mg+) • AKI Stage 2
Phase 1: Initial Management & Response
• IV Fluids (Resuscitation) • IV Electrolyte Replacement (Mg, K) • IV Ceftazidime (Empiric coverage)
✓ AKI Resolved ✓ Fast AF Resolved ✓ Inflammatory markers (CRP) improving
⚠ Diarrhea persisted ⚠ No improvement in stool frequency
Diagnostic Dilemma: Interpretation of Stool Analysis
PCR Positive (+) Toxin Negative (-)
• Indicates presence of C. diff organism (colonization potential). • Absence of free toxin suggests it may not be the primary driver of current symptoms. • HOWEVER: Patient is immunocompromised (Chemo + Pembrolizumab) with active colitis symptoms.
Decided to treat as active C. diff infection due to high clinical suspicion and host vulnerability.
Refractory Course: Escalation and Failure
1. Started Oral Vancomycin (Standard dose) 2. Escalated to Fidaxomicin + IV Metronidazole (Dual therapy) 3. Duration: Multiple days on dual therapy
Result: No improvement. Frequency increased to 18-22 episodes/day.
Endoscopic Investigation
• Procedure: Flexible Sigmoidoscopy • Visual Finding: Pseudomembranous Colitis • Action: Biopsies taken for histology & CMV IHC
Classic appearance of C. Difficile infection (yellow-white plaques). However, the patient failed maximal medical therapy for C. Diff, raising suspicion of alternative or co-pathology.
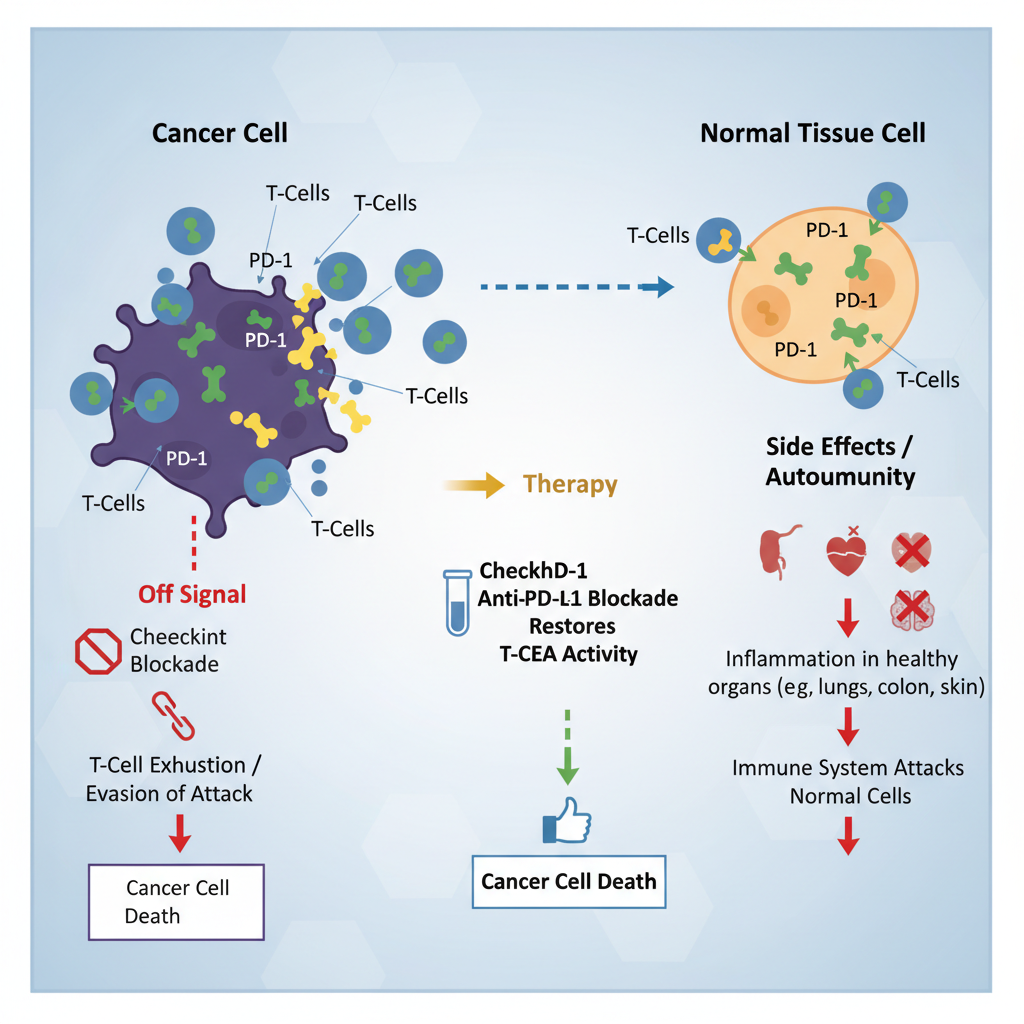
Differential 2: Pembrolizumab-Induced Colitis
• Mechanism: Immune Checkpoint Inhibitor (PD-1 blockade) unleashes T-cells, causing autoimmune-like damage to normal mucosa. • Prevalence: Colitis occurs in 2-5% of patients.
• Timing: Can occur anytime (often weeks after initiation). • Symptoms: Refractory diarrhea, abdominal pain (matches patient). • Endoscopy: Usually ulceration/inflammation, but pseudomembranes are NOT typical (though superinfection possible).
Differential 3: CMV Colitis
• Serology: IgM Weakly Positive • Significance: Suggests recent infection or reactivation (common in immunocompromised).
• Pending: CMV Nucleic Acid Detection (PCR) - Viral Load. • Pending: Biopsy Immunohistochemistry (Gold Standard).
Current Management Strategy
• STOPPED: Fidaxomicin and IV Metronidazole (Treatment Failure) • STARTED: High-Dose Oral Vancomycin (250mg every 4 hours)
• Proposed: Fecal Microbiota Transplant (FMT) • Status: Microbiology review awaited to determine suitability.
Summary & Key Takeaways
1. Complexity: Refractory diarrhea in oncology is often multifactorial (Infection vs. Toxicity).
2. Diagnostics: C. Diff PCR positive / Toxin negative presents a stewardship challenge, but immunocompromised status validates aggressive treatment.
3. Differentials: Always consider IO-Colitis (Pembrolizumab) and CMV reactivation when initial therapies fail.
- oncology
- pembrolizumab
- clostridioides-difficile
- immunotherapy-side-effects
- clinical-case-study
- medical-education