



Understanding Asthma and Albuterol: Guide & 2025 Updates
Explore asthma pathophysiology, albuterol's mechanism of action, and the latest 2024-2025 GINA clinical guidelines for respiratory care.
Asthma & Albuterol
Pathophysiology, Pharmacology, and Clinical Guidelines
Undergraduate Biology Series | 2025 Updates
What is Asthma?
Chronic Inflammatory Disorder: Airways become hypersensitive to stimuli.
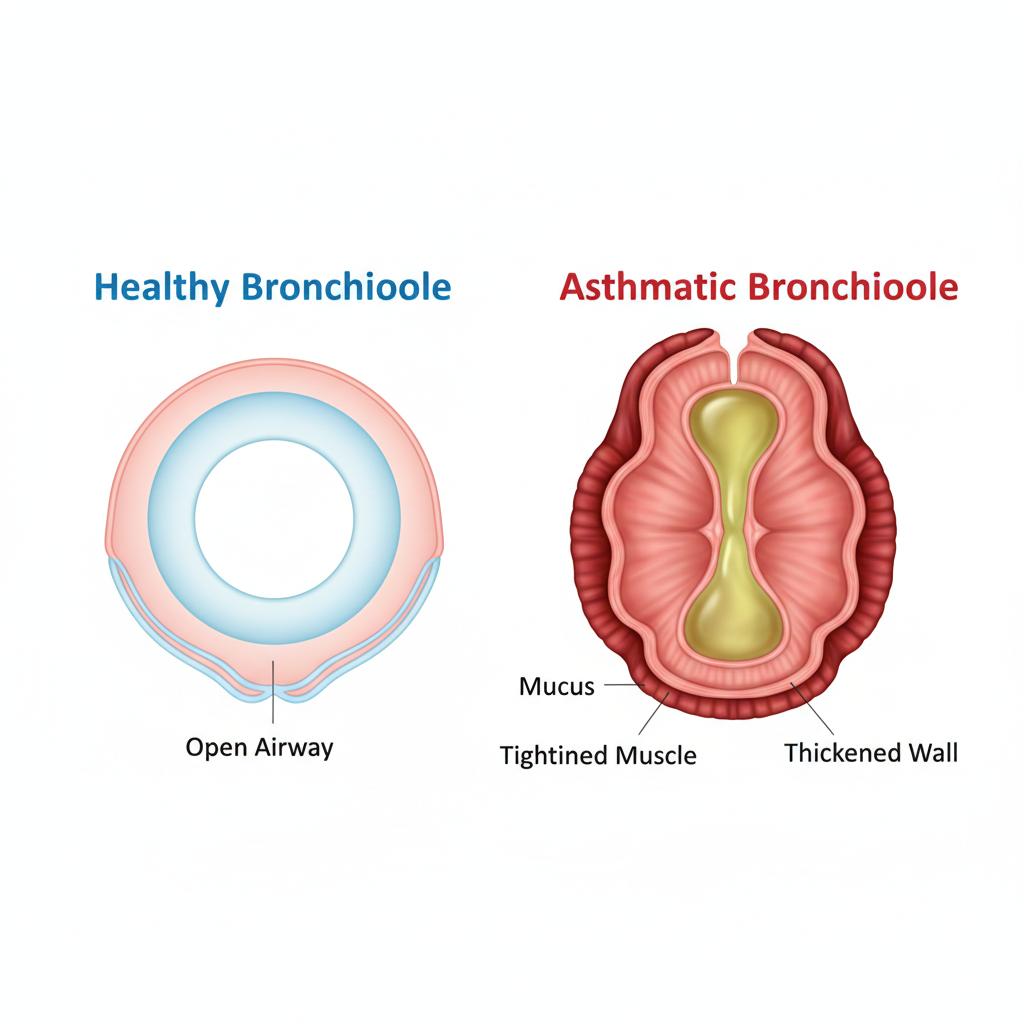
Bronchoconstriction: Smooth muscles surrounding airways tighten.
Airway Edema & Mucus: Inflammation causes swelling and excess mucus production, narrowing the lumen.
Triggers & Risk Factors
Allergens: Pollen, dust mites, pet dander, mold.
Environmental: Cold air, smoke, air pollution.
Physiological: Exercise (EIB), respiratory infections (viral), stress.
Recognizing the Symptoms
Wheezing
High-pitched whistling sound primarily during exhalation.
Shortness of Breath
Dyspnea or feeling 'air hunger'.
Chest Tightness
Feeling of heavy weight on the chest.
Coughing
Often worse at night or early morning.
Albuterol: Short-Acting Beta Agonist (SABA)
Albuterol (brand names include Ventolin, ProAir) is a bronchodilator. It is often referred to as a 'rescue inhaler' because it provides rapid relief of acute symptoms. It does NOT treat the underlying inflammation.
Drug Class: SABA
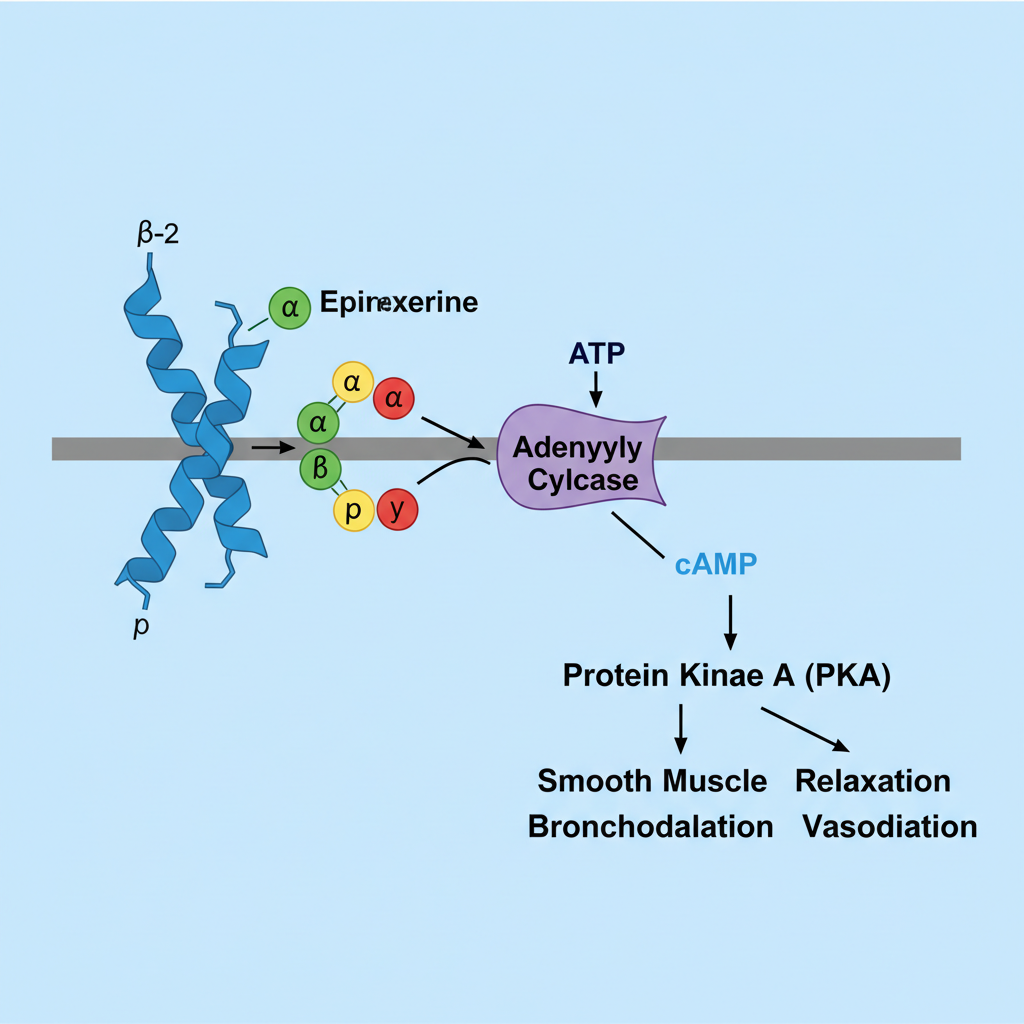
Mechanism of Action (MOA)
1. Agonist Binding: Albuterol binds selectively to Beta-2 adrenergic receptors in bronchial smooth muscle.
2. Activation: This activates adenylyl cyclase via the Gs-protein coupled pathway.
3. The Cascade: Intracellular cAMP increases, activating Protein Kinase A (PKA).
4. Result: Lower intracellular Calcium -> Smooth muscle relaxation -> Bronchodilation.
Pharmacokinetics: Onset vs. Duration
Albuterol provides rapid relief (within minutes) but the effect wears off after 4-6 hours.
CRITICAL UPDATE: 2024-2025 Guidelines
SABA-Only Therapy is No Longer Recommended
Guidelines (GINA) now advise against using Albuterol alone for adults and adolescents. Why? It treats symptoms but masks worsening inflammation. Over-reliance on SABA is linked to increased risk of severe asthma attacks. The standard of care has shifted to ICS-containing therapy.
Medication Types: Know the Difference
Rescue (Reliever)
Example: Albuterol
Relaxes muscles immediately. Used for sudden symptoms or before exercise.
Controller (Maintenance)
Example: Inhaled Corticosteroids (ICS)
Reduces inflammation over time. Must be taken daily regardless of symptoms.
Common Myths & Mistakes
MYTH: 'I only need my inhaler when I feel bad.'
FACT: Asthma is chronic. Controllers prevent attacks before they start.
ERROR: Poor Inhaler Technique
FACT: Without a spacer or proper breath-hold, medication hits the tongue/throat, not the lungs.
MYTH: 'Albuterol acts as a cure.'
FACT: It treats the symptom (constriction), not the disease (inflammation).
Side Effects & Safety
Albuterol is generally safe, but stimulating Beta-2 receptors can cause systemic effects:
Tachycardia (Fast Heart Rate)
Tremors / 'Jitteriness' (Skeletal muscle excitation)
Insomnia (if taken late at night)
Hypokalemia (Low potassium, usually only in high doses)
When to Seek Urgent Care
Red Flags Identifying an Emergency
Albuterol provides no relief or lasts < 2 hours.
Difficulty speaking in full sentences.
Retractions (skin sucking in around ribs/neck).
Cyanosis (Blue lips or fingernails) - Call 911 immediately.
- asthma
- albuterol
- pharmacology
- medical-guidelines
- rescue-inhaler
- biology
- respiratory-health