

VR and Perturbation Training for Fall Prevention Research
Explore a research proposal on VR and Perturbation-Based Balance Training (PBBT) to reduce fall risks in older adults through multimodal intervention.
VR & Perturbation Training for Fall Prevention
Research Proposal: Combating Fall Risk in Older Adults via Multimodal Intervention
Utay & Arik | BGU MSc Physiotherapy | Research Methods
Falls: A Major Public Health Challenge
Prevalence: 28% of adults over age 65 fall at least once per year.
Impact: Leading cause of ER visits and hospitalizations among seniors.
Mechanisms: Tripping, poor obstacle negotiation, gait instability, and cognitive decline.
Current Gap: Conventional strength programs fail to address complex real-world environmental demands.
The Formula of Safe Gait
Safe ambulation requires the integration of three critical systems: Cognitive, Motor, and Sensory. Deficits in executive functions like attention and decision-making directly compromise obstacle negotiation.
Intervention A: Perturbation-Based Balance Training (PBBT)
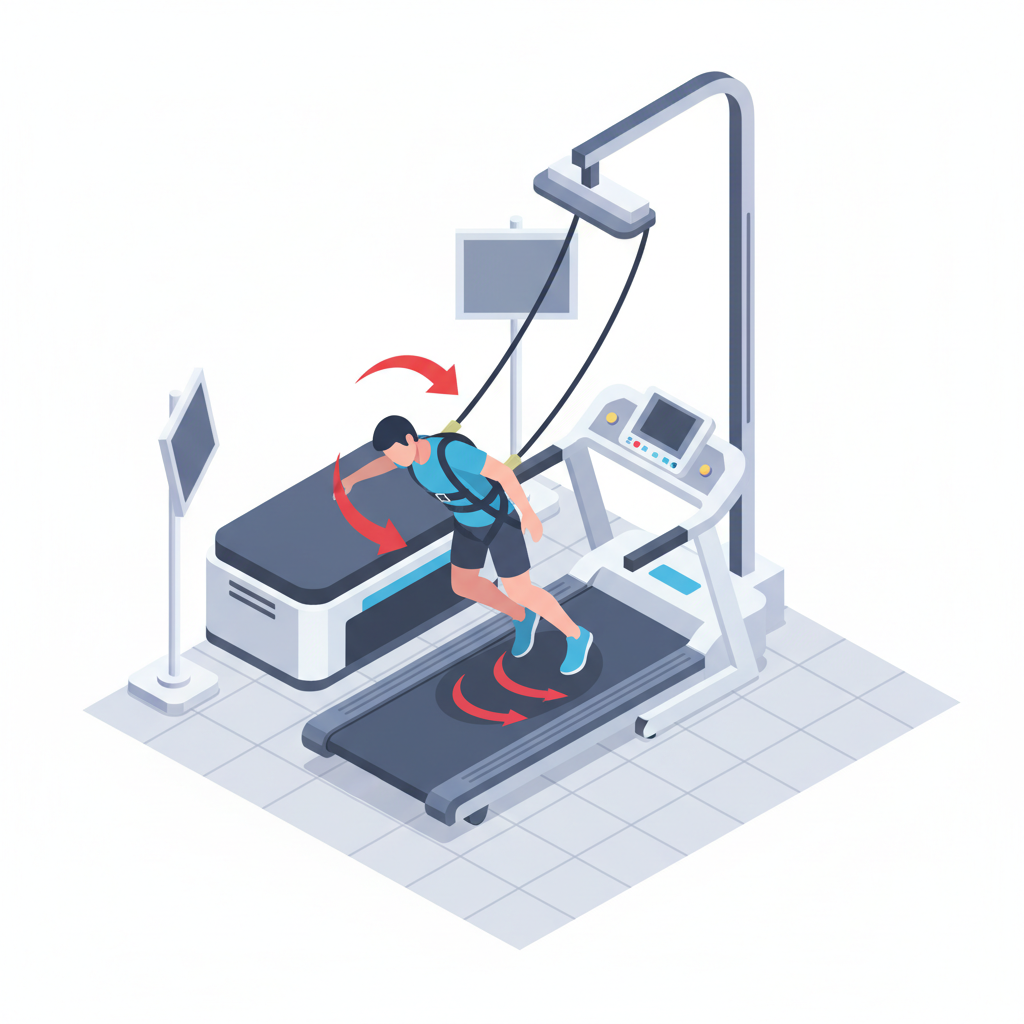
PBBT is a task-specific intervention aiming to improve reactive balance control. Participants are exposed to unannounced, multi-directional surface translations (slips/trips) in a safe environment using a harness. It targets the physical 'Motor System' response to accidental loss of balance.
Intervention B: Motor-Cognitive Training (VR-TT)
Treadmill training combined with non-immersive Virtual Reality. This dual-task environment forces the user to negotiate virtual obstacles (puddles, hurdles) while walking. It targets 'Executive Function', attention, and planning within a simulated urban or park environment.
Why Combine Them? Historical Efficacy Data
Both interventions are effective individually. VR-TT significantly reduces fall rates (IRR 0.58). PBBT reduces fall rates by ~40-46%. Combining them targets both accidental slips (PBBT) and cognitive planning (VR).
Research Question
Does the addition of a virtual reality (VR) component to Perturbation reactive balance training (PRBT) improve the effectiveness of fall prevention in high-risk older adults, compared to Perturbation reactive balance training alone?
Study Design: Prospective, Single-Blind RCT
Group 1 (Experimental): PBBT + Add-on VR training. Targets reactive response, stability, and cognitive-motor planning.
Group 2 (Control): PBBT Only. Targets reactive balance responses and postural stability.
Target: Older adults (60-90) with high fall risk (2+ falls in last 6 months).
Eligibility Criteria
INCLUSION CRITERIA
• Age 60-90 years • Fall History: 2+ falls in prior 6 months • Mobility: Can walk 5 mins unassisted • Cognition: MMSE Score > 21
EXCLUSION CRITERIA
• Psychiatric comorbidity • Neuro disorders (Stroke, TBI, PD) • Acute orthopedic pain interfering with walking • Inability to comply with protocol
Intervention Protocol
Duration: 6 weeks (18 sessions total). Frequency: 3 sessions per week. Session Length: ~30 minutes. Breakdown: 4 min Warm-up (Standard+VR), 24 min Training, 2 min Cool down. Safety: Overhead suspension harness used at all times.
Outcome Measures
PRIMARY: Incident Rate of Falls (IRR). Total falls recorded prospectively via fall calendar for 6 months post-training.
SECONDARY (Balance): Mini-BESTest and Step Execution Times. (ICC: 0.80–0.98; Ref: Horak et al., 2009)
SECONDARY (Gait): Gait speed (10m walk) and Variability during obstacle negotiation. (ICC: 0.90–0.99; Ref: Fritz & Lusardi, 2009)
SECONDARY (QoL): Falls Efficacy Scale (FES-I) for confidence and SF-36. (ICC: 0.96; Ref: Yardley et al., 2005)
Significance & Impact
This study addresses the full spectrum of fall etiology—from rapid physical failure to complex cognitive deficits. If successful, combining these high-impact modalities could establish a new, robust standard for fall prevention in rehabilitation clinics worldwide.
References
Tinetti, M. E., et al. (1988). Risk factors for falls among elderly persons living in the community. New England Journal of Medicine.
Rubenstein, L. Z. (2006). Falls in older people: epidemiology, risk factors and strategies for prevention. Age and Ageing.
Horak, F. B. (2006). Postural orientation and equilibrium: what do we need to know about neural control of balance to prevent falls? Age and Ageing.
American Geriatrics Society (2011). Summary of the Updated AGS/BGS Clinical Practice Guideline for Prevention of Falls in Older Persons.
- fall-prevention
- physiotherapy
- virtual-reality
- geriatrics
- balance-training
- clinical-research
- rehabilitation