


Behandeling Frontotemporale Dementie: Protocollen & Medicatie
Ontdek de richtlijnen voor behandeling van probleemgedrag bij FTD. Info over SSRI's, antipsychotica, GRIP-protocol en niet-farmacologische interventies.
Behandeling van Probleemgedrag bij Frontotemporale Dementie
Psychofarmaca, Hallucinaties, Emotieregulatie & Protocollen
Gebaseerd op Nederlandse richtlijnen & internationale wetenschappelijke consensus | 2026
Multidisciplinaire Richtlijn Probleemgedrag bij Dementie 2018 | ERN-RND Expert Consensus 2024 | Zorgstandaard Dementie 2026
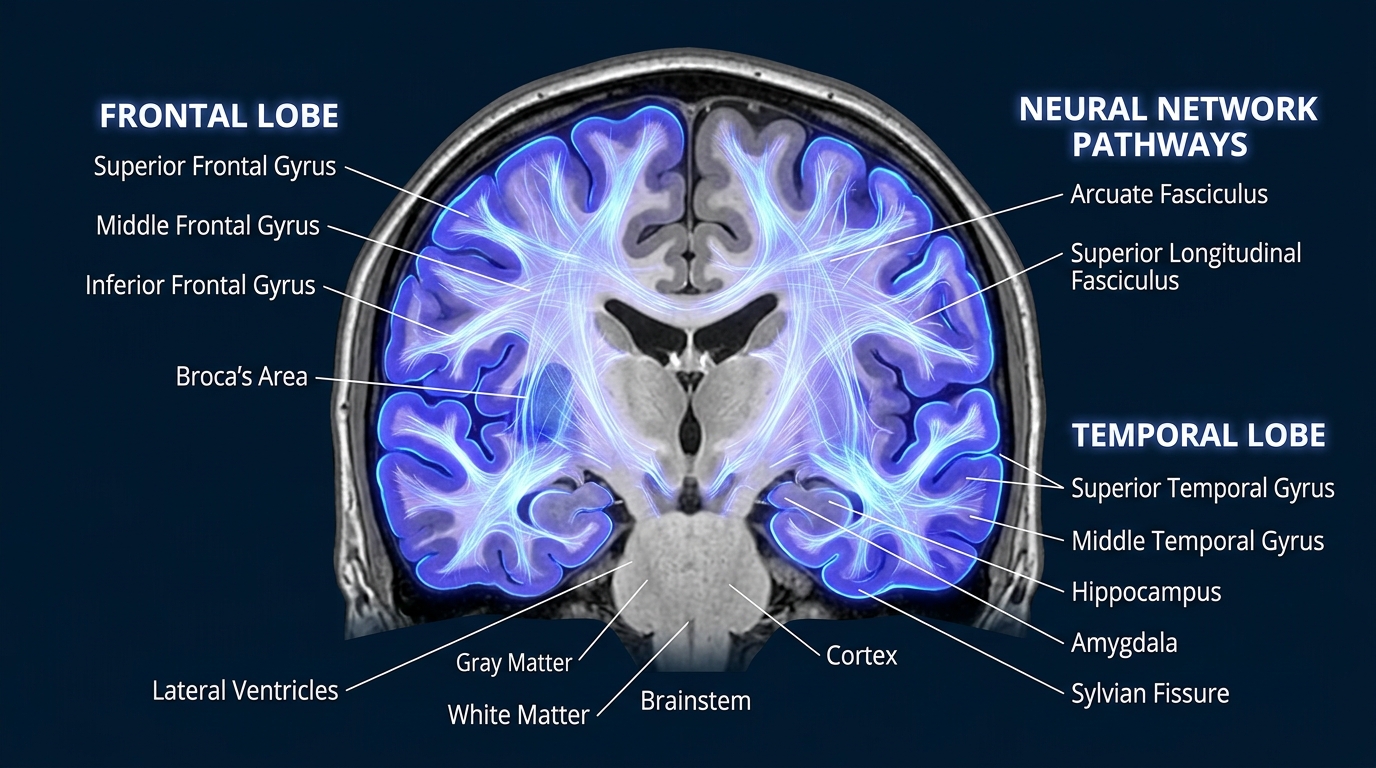
Wat is Frontotemporale Dementie?
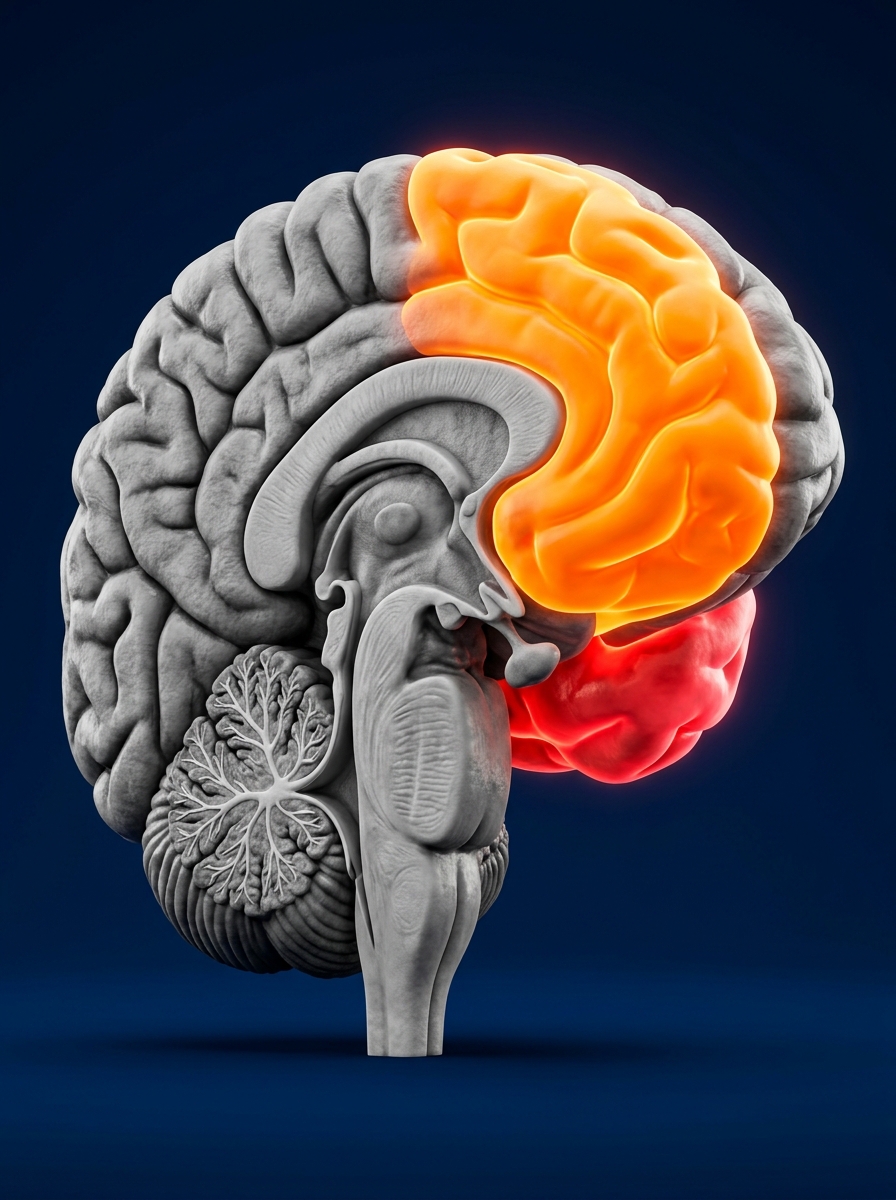
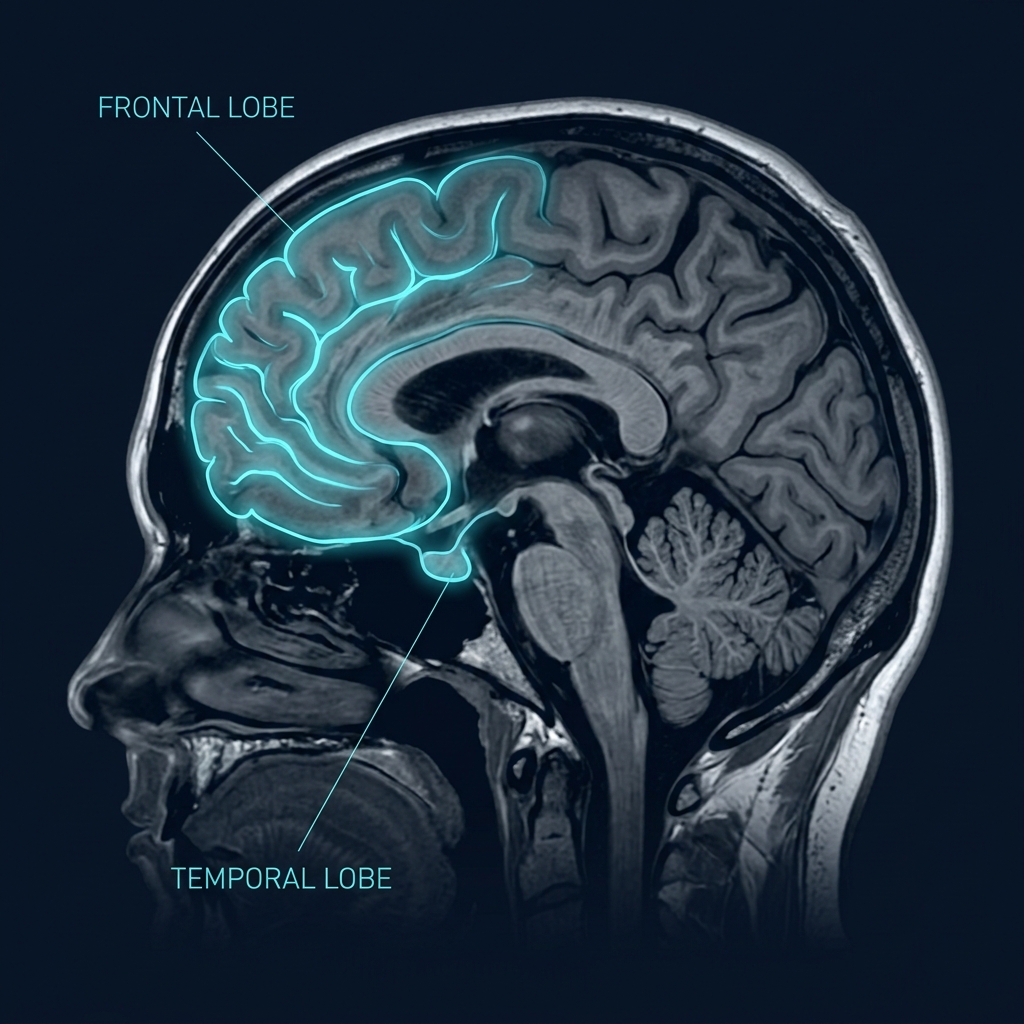
FTD is een neurodegeneratieve aandoening met atrofie van frontale en temporale kwabben. Vroege veranderingen in gedrag, persoonlijkheid en executieve functies — vaak vóór het 65e levensjaar.
Epidemiologie
~10.000 patiënten in Nederland | Meest voorkomende vroeg-onset dementie | Incidentie: 1,2 per 100.000/jaar
Pathologie
TDP-43, tau of FUS eiwitophopingen | Frontale en temporale corticale degeneratie | Genetisch in ~40% (C9orf72, GRN, MAPT)
Klinische varianten
bvFTD (gedragsvariant) | Semantische dementie | Niet-vloeiende/agrammatische afasie
Bron: Rascovsky et al. 2011 | Amsterdam UMC | Erasmus MC | Zorgstandaard Dementie 2026
Frontale kwab (aangetast)
Temporale kwab (aangetast)
Probleemgedrag bij FTD: Kernsymptomen
Ontremming
Impulsiviteit, ongepast sociaal gedrag, stelen, seksuele ontremming
Apathie
Verlies van motivatie, initiatiefverlies, emotionele vlakheid, teruggetrokkenheid
Dwangmatigheid
Stereotiep gedrag, rigide routines, hamsteren, hyperfagie
Empathieverlies
Gebrek aan inlevingsvermogen, sociale ontkoppeling, egocentrisch gedrag
Agressie
Verbale of fysieke agressie, agitatie, prikkelbaarheid bij weerstand
Executief disfunctioneren
Moeite met plannen, oordelen, flexibiliteit en zelfinzicht
NPI-Q Screening
Elke 6 maanden aanbevolen (GRIP-protocol)
Bron: Internationale consensus criteria bvFTD (Rascovsky et al., 2011) | NPI-Q Cummings et al.
Auditieve & Visuele Hallucinaties
Hallucinaties bij 3–25% van FTD-patiënten. Minder frequent dan bij Lewy body dementie, maar klinisch significant.
Auditieve hallucinaties
Stemmen, geluiden, muziek — gelinkt aan atrofie van de superieure temporale gyrus
Visuele hallucinaties
Beelden, personen — geassocieerd met rechter hemisfeer en anterieure cingulate atrofie
TDP-43 aggregatie → verstoring serotoninerge en dopaminerge neurotransmissie → verlaagde inhibitie → perceptuele ontregeling
Emotieregulatieproblemen
Frontale atrofie leidt tot disfunctioneren van het orbitofrontale cortex–amygdala circuit:
Labiele affect (snelle stemmingswisselingen)
Verminderde frustratie-tolerantie
Explosieve uitbarstingen bij kleine prikkels
Verlies van sociale filtering (geen remming)
Verlies van angstrespons (amygdala dysfunctie)
Bron: Lanata & Miller 2016 | Rascovsky et al. 2011 | ERN-RND Expert Consensus 2024
GRIP-Protocol: Methodische Aanpak Probleemgedrag
Grip op Probleemgedrag bij Dementie | VUmc/Radboudumc 2014
01
Signalering
NPI-Q screening elke 6 maanden
Vroeg vaststellen gedragssymptomen
Observatie door verzorgend team
02
Analyse
Multidisciplinair werkblad
Arts en psycholoog
Oorzaakanalyse: somatisch, psychisch, omgeving
03
Behandeling
Eerst psychosociale interventies
Structuur en prikkelreductie
Psychofarmaca alleen indien nodig
04
Evaluatie
Wekelijks monitoren eerste maand
Afbouw na 3 maanden
Stoppoging verplicht, consulteer CCE
GRIP-methode | Multidisciplinaire Richtlijn 2018 | Vilans Kenniscentrum
Niet-Farmacologische Interventies
Eerste keuze behandeling — altijd vóór psychofarmaca
Omgevingsinterventies
<ul style="margin: 0; padding-left: 30px; list-style-type: none; display: flex; flex-direction: column; gap: 35px;"> <li style="font-size: 25px; color: #ffffff; line-height: 1.4; position: relative;"> <span style="position: absolute; left: -30px; color: #87cefa; font-weight: bold; font-size: 28px;">•</span> Prikkelreductie: rustige omgeving. </li> <li style="font-size: 25px; color: #ffffff; line-height: 1.4; position: relative;"> <span style="position: absolute; left: -30px; color: #87cefa; font-weight: bold; font-size: 28px;">•</span> Vaste dagstructuur en routine. </li> <li style="font-size: 25px; color: #ffffff; line-height: 1.4; position: relative;"> <span style="position: absolute; left: -30px; color: #87cefa; font-weight: bold; font-size: 28px;">•</span> Aangepaste woonruimte (licht, kleur). </li> <li style="font-size: 25px; color: #ffffff; line-height: 1.4; position: relative;"> <span style="position: absolute; left: -30px; color: #87cefa; font-weight: bold; font-size: 28px;">•</span> Vermijden van uitlokkende situaties. </li> </ul>
Persoonsgerichte Zorg
<ul style="margin: 0; padding-left: 30px; list-style-type: none; display: flex; flex-direction: column; gap: 35px;"> <li style="font-size: 25px; color: #ffffff; line-height: 1.4; position: relative;"> <span style="position: absolute; left: -30px; color: #86efac; font-weight: bold; font-size: 28px;">•</span> Validatie en reminiscentietherapie. </li> <li style="font-size: 25px; color: #ffffff; line-height: 1.4; position: relative;"> <span style="position: absolute; left: -30px; color: #86efac; font-weight: bold; font-size: 28px;">•</span> Muziektherapie bij agitatie. </li> <li style="font-size: 25px; color: #ffffff; line-height: 1.4; position: relative;"> <span style="position: absolute; left: -30px; color: #86efac; font-weight: bold; font-size: 28px;">•</span> Zinvolle dagbesteding. </li> <li style="font-size: 25px; color: #ffffff; line-height: 1.4; position: relative;"> <span style="position: absolute; left: -30px; color: #86efac; font-weight: bold; font-size: 28px;">•</span> Mantelzorgondersteuning en psycho-educatie. </li> </ul>
Communicatiestrategieën
<ul style="margin: 0; padding-left: 30px; list-style-type: none; display: flex; flex-direction: column; gap: 35px;"> <li style="font-size: 25px; color: #ffffff; line-height: 1.4; position: relative;"> <span style="position: absolute; left: -30px; color: #d8b4fe; font-weight: bold; font-size: 28px;">•</span> Eenvoudige, korte instructies. </li> <li style="font-size: 25px; color: #ffffff; line-height: 1.4; position: relative;"> <span style="position: absolute; left: -30px; color: #d8b4fe; font-weight: bold; font-size: 28px;">•</span> Non-verbale communicatie. </li> <li style="font-size: 25px; color: #ffffff; line-height: 1.4; position: relative;"> <span style="position: absolute; left: -30px; color: #d8b4fe; font-weight: bold; font-size: 28px;">•</span> Kalmerende benadering. </li> <li style="font-size: 25px; color: #ffffff; line-height: 1.4; position: relative;"> <span style="position: absolute; left: -30px; color: #d8b4fe; font-weight: bold; font-size: 28px;">•</span> Vermijden van confrontatie. </li> </ul>
Psychofarmaca pas overwegen na falen van niet-farmacologische interventies (Richtlijn 2018)
Zorgstandaard Dementie 2026 | Multidisciplinaire Richtlijn 2018
Psychofarmaca bij Frontotemporale Dementie
Symptomatisch — geen curatieve werking | Altijd na niet-farmacologische interventies
GECONTRA-INDICEERD BIJ FTD
Cholinesteraseremmers (donepezil etc.) zijn GECONTRA-INDICEERD bij FTD — kunnen symptomen verergeren
ERN-RND Expert Consensus 2024 | Nederlandse Richtlijn Probleemgedrag 2018
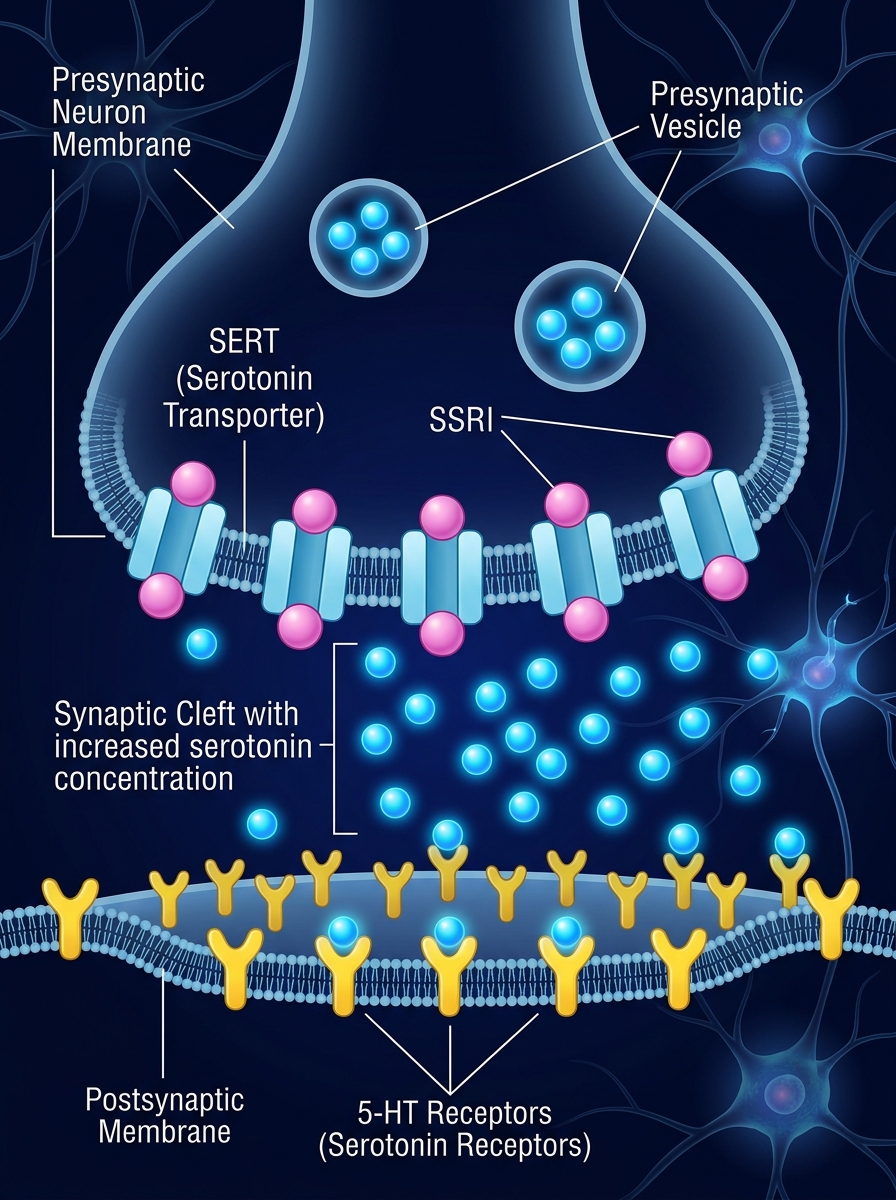
SSRI's — Eerste Keuze bij FTD
Selectieve Serotonine Heropname Remmers
SSRI's blokkeren SERT in de presynaptische neuron. Serotonine blijft langer beschikbaar in de synaptische spleet — verbeterde neurotransmissie in orbitofrontaal circuit.
Indicaties bij FTD
Ontremming en impulsiviteit
Obsessief-compulsief gedrag
Hyperfagie
Stereotiep gedrag
Emotionele labiliteit
⚠ Nausea, QTc-verlenging bij citalopram >40mg, hyponatriëmie
ERN-RND 2024 | Richtlijn 2018
Presynaptisch
SERT geblokkeerd
Serotonine
Postsynaptisch
5-HT Receptor
Antipsychotica bij FTD
Tweede keuze — alleen bij ernstige agressie of veiligheidsrisico's
Quetiapine
Atypisch antipsychoticum
Indicatie: ernstige agressie, nachtelijke onrust, psychose bij FTD
Startdosering: 12,5–25 mg/dag
Werkingsmechanisme: D2 en 5-HT2A receptor antagonisme
Voordeel: laag EPS-risico
Olanzapine
Indicatie: ernstige agitatie indien quetiapine onvoldoende
Dosering: 2,5–5 mg/dag
Breed receptorprofiel: D1-4, 5-HT2, H1, muscarine
Bijwerkingen: gewichtstoename, metabole effecten
RISICO'S & WAARSCHUWINGEN
⚠ Verhoogde mortaliteit (+1,6–1,7x bij dementie)
⚠ Cerebrovasculaire events (CVA-risico)
⚠ Val- en fractuurrisico
⚠ Parkinsonisme en sedatie
⚠ QTc-verlenging
❌ FDA Black Box Warning ouderen met dementie
Gebruik laagst effectieve dosis | Evalueer na 4–6 weken | Afbouwen na 3 maanden (Richtlijn 2018)
FDA Black Box Warning | ERN-RND 2024 | NL Richtlijn 2018
Trazodon & Mirtazapine bij FTD
Effectieve opties voor agitatie, motorische onrust en slaapproblemen
Trazodon
Serotonine Antagonist & Heropname Remmer (SARI)
Blokkeert 5-HT2A receptoren én remt serotonine heropname. Resulteert in sederende én serotonerg activerende werking.
Motorische onrust / agitatie
Slaapstoornissen
Prikkelbaarheid
Mild gedragsmatige ontremming
50–300 mg/dag (laag starten, 's avonds)
Duizeligheid, orthostatische hypotensie, sedatie
Meerdere open-label studies tonen effectiviteit bij FTD-agitatie (Lebert et al., 2004)
Mirtazapine
Noradrenerge en Specifieke Serotoninerge Antidepressivum (NaSSA)
Blokkeert α2-receptoren (verhoogt noradrenaline/serotonine afgifte) + blokkeert H1 (sterk sederend) + 5-HT2/3 antagonisme
Ernstige slaapproblemen
Nachtelijke onrust en agitatie
Gewichtsverlies/eetproblemen
Angst en prikkelbaarheid
7,5–15 mg voor de nacht (lage dosis = meer sedatie)
Sterke sedatie, gewichtstoename, droge mond
Voorkeur: Trazodon voor dagelijks gebruik | Mirtazapine voor nachtelijke problemen | Geen verhoogd mortaliteitsrisico zoals bij antipsychotica ✅
ERN-RND Expert Consensus 2024 | Lebert et al. 2004 | Camprodon-Boadas et al. 2022
Apathie bij FTD: Een Onderschat Probleem
Meest invaliderende symptoom — moeilijkste te behandelen
ERN-RND 2024 | Padala et al. 2018 | Multidisciplinaire Richtlijn 2018
Behandelprotocol Probleemgedrag FTD
Multidisciplinaire Richtlijn 2018 & Zorgstandaard Dementie 2026
🔍 <span style='color: #60a5fa;'>STAP 1:</span> Signalering via NPI-Q score — vroegtijdig vaststellen probleemgedrag
Aanwijsbare lichamelijke oorzaak?<br><span style='font-size: 13px; font-weight: 400; color: #94a3b8;'>(pijn, infectie, medicatie)</span>
Behandel onderliggende oorzaak eerst
💬 <span style='color: #60a5fa;'>STAP 2:</span> Start niet-farmacologische interventies (4 weken)<br><span style='font-size: 16px; font-weight: 400; color: #93c5fd;'>Structuur • Prikkelreductie • Communicatieaanpassing</span>
Voldoende effect<br>na 4 weken?
✅ Continueer — heranalyseer elke 6 maanden
💊 <span style='color: #c084fc;'>STAP 3:</span> Start psychofarmaca op indicatie<br><span style='font-size: 16px; font-weight: 400; color: #e9d5ff;'>SSRI bij ontremming/dwang | Trazodon bij agitatie | Quetiapine bij agressie</span>
📊 <span style='color: #fbbf24;'>STAP 4:</span> Wekelijks monitoren eerste maand — effect en bijwerkingen evalueren
✅ <span style='color: #34d399;'>STAP 5:</span> Laagste effectieve dosis handhaven — afbouwen na 3 maanden — stoppoging verplicht
<strong style='color:#38bdf8; font-size: 18px;'>CCE</strong><br>Centrum voor Consultatie en Expertise
<strong style='color:#f43f5e; font-size: 18px;'>Chronisch gebruik psychofarmaca:</strong><br>NIET aanbevolen
<strong style='color:#fbbf24; font-size: 18px;'>Afbouwen:</strong><br>Altijd in overleg met behandelend arts
Multidisciplinaire Richtlijn Probleemgedrag bij Dementie 2018 | Zorgstandaard Dementie 2026
Samenvatting: Kernpunten Behandeling FTD
FTD ≠ Alzheimer
Specifieke aanpak vereist. Cholinesteraseremmers zijn gecontra-indiceerd. Andere farmacologie!
Niet-farmacologisch eerst
Structuur, prikkelreductie en persoonsgerichte zorg zijn altijd de eerste stap (GRIP-protocol)
SSRI's = Eerste keuze
Bij ontremming, dwang en impulsiviteit. Citalopram of sertraline als voorkeursbehandeling
Antipsychotica = Laatste redmiddel
Quetiapine alleen bij ernstige agressie/veiligheidsrisico. Laag doseren, kort gebruiken, monitoren
Altijd evalueren en afbouwen
Wekelijks monitoren eerste maand. Stoppoging na 3 maanden. Chronisch gebruik vermijden
Multidisciplinaire aanpak
Arts, psycholoog, verpleegkundige, mantelzorger en CCE bij complexe situaties betrekken
Multidisciplinaire Richtlijn Probleemgedrag bij Dementie 2018 | ERN-RND Expert Consensus 2024 | Zorgstandaard Dementie 2026 | GRIP-methode VUmc/Radboudumc
- frontotemporale-dementie
- ftd
- geronto-psychiatrie
- neuropsychologie
- grip-methode
- psychofarmaca
- zorgstandaard-dementie