

Pathophysiology of Diabetic Foot for Nurses | Bobr.ai
Learn the mechanisms of diabetic foot disease, including neuropathy, angiopathy, and Charcot foot, with clinical screening tools and patient education tips.
Pathophysiology of Diabetic Foot
How Diabetes Affects the Feet & Its Complications
Jawaher Almaskari
Podiatrist | Seeb Polyclinic
Presented for Health Centre Nurses
What is Diabetic Foot Disease?
A serious complication of diabetes affecting the feet
Includes: neuropathy, poor circulation, ulcers, infections & amputation
15–25%
Lifetime risk of foot ulcer in diabetics
50–70%
Ulcer recurrence rate within 5 years
Up to 85%
of amputations are preceded by a foot ulcer
How Does Diabetes Damage the Feet?
4 Main Pathophysiological Mechanisms
Metabolic Dysfunction
Hyperglycemia damages nerves and blood vessels
Nerve Damage (Neuropathy)
Loss of feeling, weakness, dry skin
Blood Vessel Disease (Angiopathy)
Poor circulation, atherosclerosis
Immune Impairment
Reduced ability to fight infections
These 4 factors together lead to
Diabetic Foot Ulcers, Infections & Amputation
Diabetic Neuropathy
Loss of Feeling
SENSORY NEUROPATHY
Loss of protective sensation — patient can't feel pain, heat, pressure → injuries go unnoticed
MOTOR NEUROPATHY
Muscle weakness → foot deformities (claw toes, hammer toes) → abnormal pressure points
AUTONOMIC NEUROPATHY
Dry skin, no sweating → cracked skin, fissures → entry point for infection
Neuropathy is the underlying cause in >60% of diabetic foot ulcers
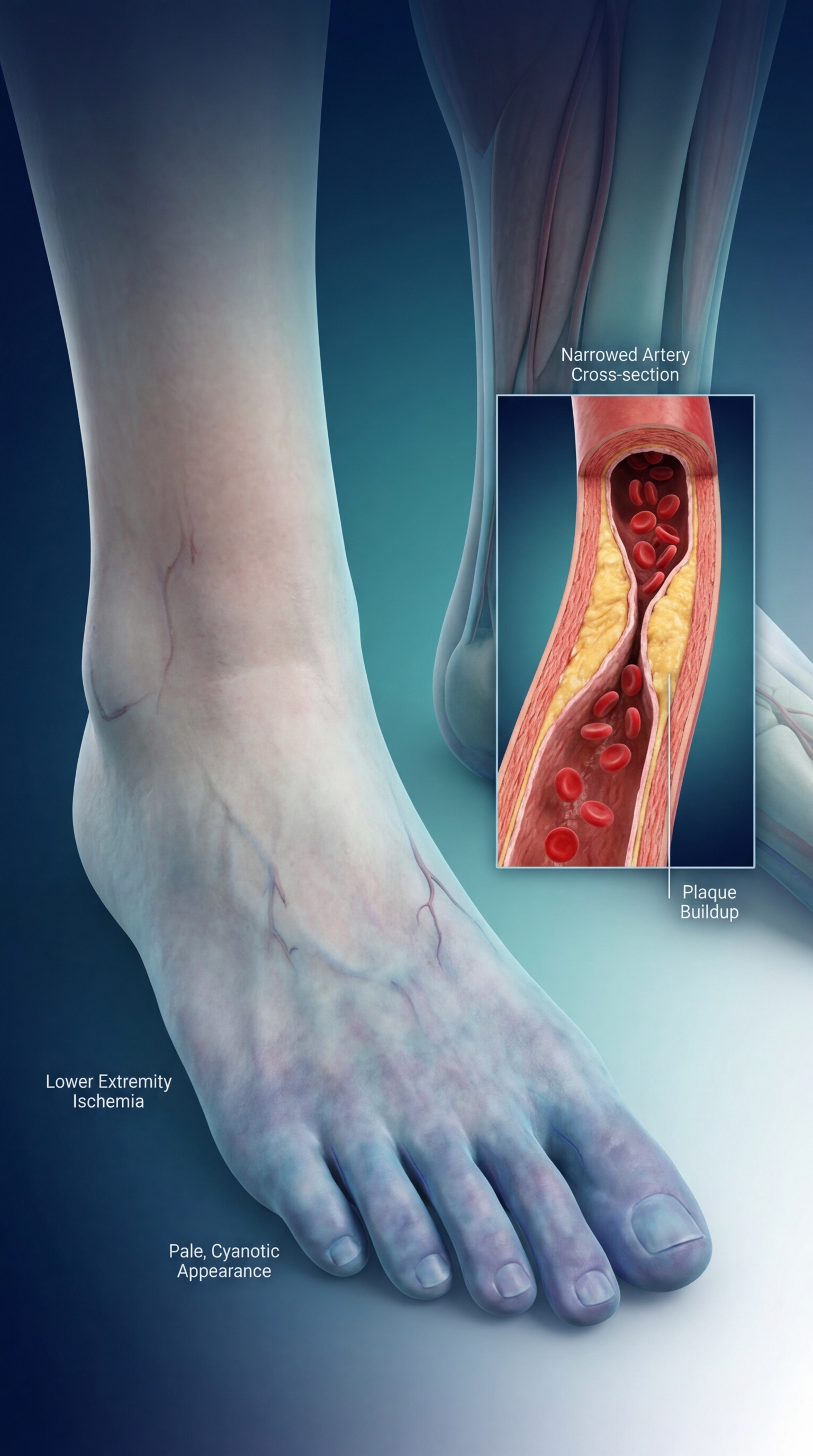
Poor Blood Flow — Diabetic Angiopathy
Can lead to: ischemia → gangrene → amputation
Signs to watch for
Absent foot pulses, cold feet, pale/blue skin, pain on walking
How Ulcers Develop — The Pathway to Ulceration
Diabetes → Neuropathy
Nerve damage causes a profound loss of sensation in the feet.
Pressure & Deformities
Abnormal foot pressure and structural changes cause callus formation.
Subcutaneous Bleeding
Callus builds up over time, triggering bleeding under the skin.
Foot Ulcer
Skin breaks down entirely, exposing deeper tissues.
Minor trauma (e.g., tight shoes, walking barefoot) → Unnoticed due to neuropathy → Foot Ulcer
The patient often does NOT feel pain — which is why regular foot inspection is critical!
Diabetic Foot Infections
High blood sugar impairs white blood cell function
Poor circulation limits antibiotic delivery to tissues
Loss of sensation = infections go unnoticed
Skin cracks and ulcers = entry points for bacteria
Most common: Staphylococcus aureus
MRSA found in up to 30% of cases
Severe infections can reach bone (Osteomyelitis)
⚠️ Infection in a diabetic foot = EMERGENCY — can spread rapidly to bone and blood, leading to amputation
Charcot Foot
A Special Complication
What is it?
A progressive bone and joint destruction in the foot
Caused by: neuropathy + increased blood flow + repeated minor trauma
Bones weaken and fracture without pain
What does it look like?
Red, hot, swollen foot (can mimic infection)
Midfoot collapse → 'rocker-bottom' foot deformity
Foot becomes very deformed over time
Why is it important for nurses to know?
Easy to miss — patient has NO pain due to neuropathy
Must be differentiated from infection
Early detection and offloading prevents severe deformity
KEY SIGN:
Hot, swollen foot in a diabetic patient with neuropathy = suspect Charcot foot
Risk Stratification — Who Is at High Risk?
IWGDF Risk Categories for Clinical Screening
Risk Level
Description
Check Frequency
0 — Very Low
No neuropathy, no PAD
Once a year
1 — Low
Neuropathy OR poor circulation
Every 6–12 months
2 — Moderate
Neuropathy + poor circulation OR foot deformity
Every 3–6 months
3 — High
History of ulcer or amputation + neuropathy/PAD
Every 1–3 months
LOPS = Loss of Protective Sensation (tested with 10g monofilament)
PAD = Peripheral Artery Disease (check foot pulses)
All diabetic patients need annual foot screening — even those with no symptoms!
The Nurse's Role — Foot Screening Checklist
What to LOOK for
Skin colour and temperature changes
Callus, blisters, fissures or wounds
Nail problems (ingrown, fungal, thickened)
Foot deformities (claw toes, bunions)
Swelling or redness
What to TEST
<span style="color: #FFFFFF; font-weight: 600;">Sensation:</span> 10g monofilament test (3 sites per foot)
<span style="color: #FFFFFF; font-weight: 600;">Pulses:</span> Dorsalis pedis and posterior tibial
<span style="color: #FFFFFF; font-weight: 600;">Footwear:</span> Check inside shoes for rough edges
<span style="color: #FFFFFF; font-weight: 600;">Skin moisture:</span> Dry vs normal
<span style="color: #FFFFFF; font-weight: 600;">Ask about:</span> Numbness, tingling, pain on walking
Refer to podiatry if:
ulcer present, LOPS confirmed, absent pulses, Charcot suspected, or foot deformity found
Patient Education
Key Messages for Diabetic Patients
👣
Inspect both feet daily — look between the toes
🚿
Wash feet daily in warm water (below 37°C), dry well between toes
👟
Never walk barefoot — indoors or outdoors
🩺
Wear properly fitting shoes — check inside before putting on
🧴
Moisturize dry skin — but NOT between toes
✂️
Cut toenails straight across
🌡️
Never use hot water bottles on feet
🏥
Report any wound, blister or color change immediately
Early reporting saves limbs. A small cut can become a major problem in a diabetic patient.
Key Takeaways
Diabetes causes nerve damage, poor circulation and immune impairment — all affecting the feet
Neuropathy = patient feels NO pain → injuries go unnoticed → ulcers develop
Poor blood flow = wounds heal slowly → risk of gangrene and amputation
All diabetic patients need annual foot screening — even without symptoms
Early detection and prompt referral can prevent amputation
Questions?
Contact Jawaher Almaskari — Podiatrist, Seeb Polyclinic
- diabetic-foot
- pathophysiology
- nursing-education
- diabetes-complications
- neuropathy
- podiatry
- clinical-screening
- healthcare