Acyanotic Congenital Heart Diseases & Coarctation of Aorta
Deep dive into Acyanotic CHD, Coarctation of Aorta (CoA), duct-dependent lesions, and emergency neonatal management for MD, DNB, and MRCPCH exams.
PAEDIATRIC CARDIOLOGY
Acyanotic Congenital Heart Diseases
with Focus on Coarctation of Aorta
Presented by
Dr. Ajinkya Kale
MBBS, MD Paediatrics
Neonatal Fellow (UK)
Lactation Consultant (BPNI, AIIMS Nagpur)
2026
What is Cyanosis?
Recognizing clinical signs & presentation
Acyanotic CHD — Classification & Examples
Left-to-right shunts & major subtypes
Coarctation of Aorta — Deep Dive
Pathophysiology, hemodynamics & diagnosis
Duct-Dependent Lesions
Prostaglandin use & critical stabilization
Emergency Management
Acute care & initial stabilization protocols
Definitive Surgical Management
Repair timing & operative approaches
India Statistics & Burden
Epidemiology & regional healthcare challenges
Key Pearls, Viva Q&A & Closing
Important takeaways & interactive review
FUNDAMENTALS
What is Cyanosis?
Cyanosis is the bluish-purple discolouration of the skin and mucous membranes caused by increased concentration of deoxygenated haemoglobin (>5 g/dL) in capillary blood.
CENTRAL CYANOSIS
Affects tongue, lips, mucous membranes. Indicates systemic desaturation. SpO2 typically <85%.
PERIPHERAL CYANOSIS
Affects extremities only. Can be normal in newborns (acrocyanosis).
Cyanosis is NOT always pathological in newborns — acrocyanosis in first 24-48 hrs is normal!
Acyanotic Congenital Heart Diseases
Left-to-Right Shunts & Obstructive Lesions
Left-to-Right Shunts
VSD (Ventricular Septal Defect)
Most common CHD, ~32%
ASD (Atrial Septal Defect)
Ostium secundum most common
PDA (Patent Ductus Arteriosus)
Common in premature infants
AVSD (Atrioventricular Septal Defect)
Associated with Down syndrome
PAPVR
Partial Anomalous Pulmonary Venous Return
Obstructive Lesions
Today's Focus
Coarctation of Aorta (CoA)
Narrowing of the descending aorta
Pulmonary Stenosis (PS)
Obstruction of right ventricular outflow tract
Aortic Stenosis (AS)
Obstruction of left ventricular outflow tract
Hypoplastic Left Heart Syndrome (HLHS)
Severe underdevelopment of left heart structures
📌 Acyanotic = No right-to-left shunt. May become cyanotic if Eisenmenger develops.
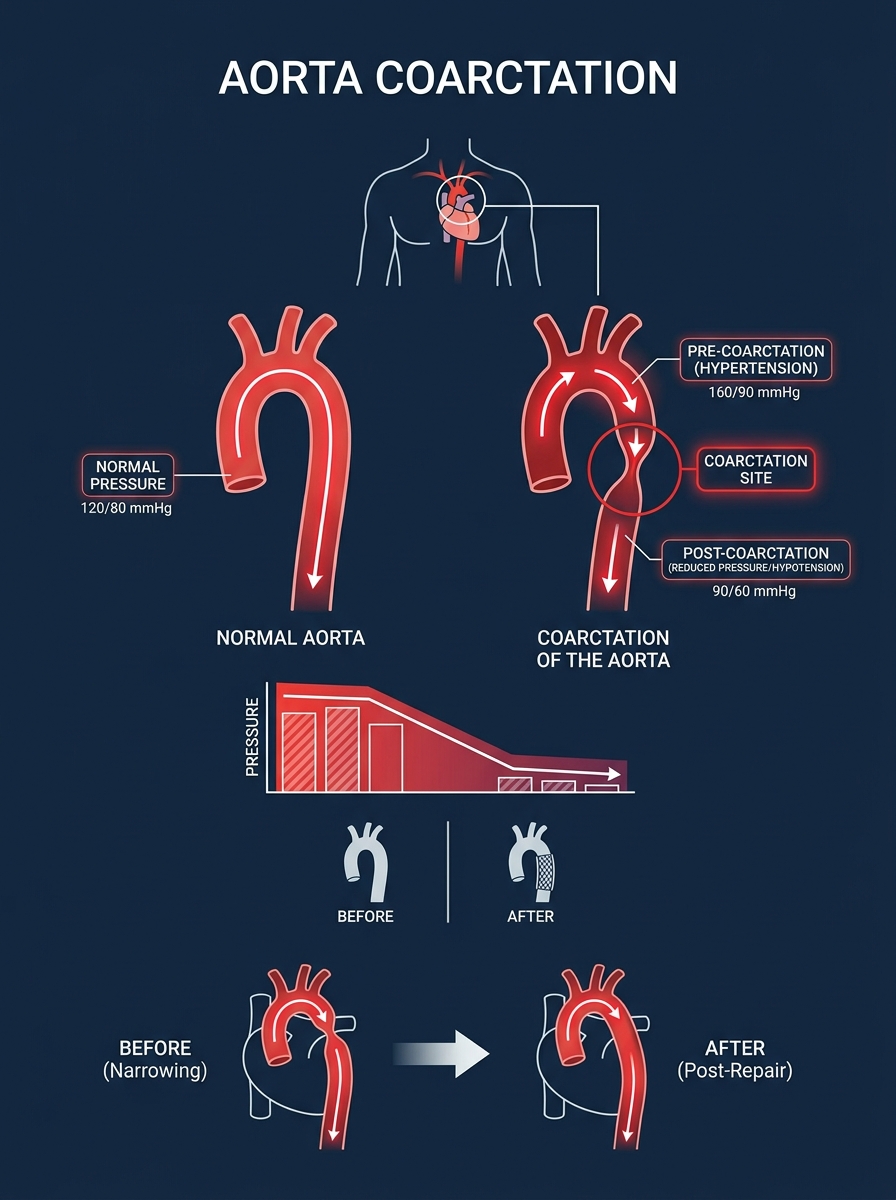
COARCTATION OF AORTA
Narrowing That Can Kill
Coarctation of the Aorta (CoA) is a discrete narrowing of the aortic lumen, most commonly at or just distal to the ductus arteriosus (juxtaductal), causing obstruction to blood flow.
Juxtaductal (near ligamentum arteriosum) — just distal to origin of left subclavian artery
Duct-Dependent Lesions
When the ductus closes — the baby crashes
What is the Ductus?
The ductus arteriosus connects pulmonary artery to descending aorta
Normally closes within 24-72 hours after birth
Mediated by rise in O₂, fall in prostaglandins
Duct-Dependent Systemic Flow
Lesions where systemic flow DEPENDS on PDA:
Coarctation of Aorta (critical)
Interrupted Aortic Arch
Hypoplastic Left Heart Syndrome (HLHS)
Critical Aortic Stenosis
These babies present with SHOCK when PDA closes
Duct-Dependent Pulmonary Flow
Lesions where pulmonary flow DEPENDS on PDA:
Pulmonary Atresia
Tricuspid Atresia
Critical Pulmonary Stenosis
Tetralogy of Fallot (severe)
These babies present with SEVERE CYANOSIS when PDA closes
GOLDEN RULE: Any neonate presenting in shock or severe cyanosis in first week of life = THINK DUCT-DEPENDENT LESION → Start PGE1 IMMEDIATELY
Definitive Surgical Management
Coarctation of Aorta — Timing & Techniques
Surgical Options
RESECTION & END-TO-END ANASTOMOSIS
<b>Gold standard in neonates and infants.</b> Resect the coarcted segment + extended anastomosis. Low recurrence rate. <b>Approach:</b> Left posterolateral thoracotomy.
SUBCLAVIAN FLAP AORTOPLASTY
Uses left subclavian artery as a flap to widen the coarctation. Useful in very small neonates. <b>Disadvantage:</b> May compromise left arm blood flow.
PATCH AORTOPLASTY
Dacron/Gore-Tex patch to widen segment. Higher risk of aneurysm formation — less preferred.
BALLOON ANGIOPLASTY ± STENTING
Preferred in older infants, children, adolescents and <b>RECOARCTATION</b>. Stents in children >25kg. <b>Risks:</b> Aneurysm, dissection.
Timing of Surgery
<b>Symptomatic neonate:</b> URGENT surgery (within 24-48h of stabilization)
<b>Asymptomatic infant:</b> Elective at 3-6 months
<b>Older child/adolescent:</b> At diagnosis
Complications to Watch
Recoarctation (10-15% in neonates)
Paradoxical hypertension post-op
Spinal cord ischemia (rare)
Recurrent laryngeal nerve injury
Chylothorax
Long-term Follow-up
Monitor BP in all 4 limbs annually
Echocardiography every 1-2 years
MRI aorta in adulthood
Lifelong cardiology follow-up
CHD in India — The Numbers
A Crisis We Can No Longer Ignore
240,000
New babies born with CHD every year in India
1 in 100
Newborns affected by congenital heart disease
25-30%
Of affected children die before age 1 without intervention
9.8%
Of ALL infant deaths in India attributed to Critical CHD (2018-2021)
<20%
Of children with CHD actually receive any form of cardiac care
28%
of all birth defect-related deaths in India are due to CHD — making it the #1 killer among birth defects
The Problem
Only ~50 paediatric cardiac surgery centres exist in a country of 1.4 billion people
The Hope
With timely PGE1 + referral, survival rates can exceed 90% post-surgery
PAEDIATRIC CARDIOLOGY
Saving a Life — It's Simpler Than You Think
The Chain of Survival in Duct-Dependent CHD
You — the first doctor who examines this baby — are the most important link in this chain.
WITHOUT RECOGNITION:
Baby dies of refractory shock within hours to days
WITH PGE1 + TIMELY SURGERY:
Child grows up, plays sports, lives a full life
RECOGNISE
Weak femoral pulses, shock, pre/post-ductal SpO₂ difference, sick neonate day 2-5
START PGE1
0.05 mcg/kg/min IV — Within minutes, perfusion is restored
CALL & TRANSFER
Contact nearest cardiac centre. Stable baby on PGE1 travels safely
SURGERY
Resection & end-to-end anastomosis. Median operating time: 2-3 hours
SURVIVOR
90%+ survival post-surgery. Normal life expectancy with follow-up
Key Clinical Pearls
Things That Will Save Lives & Ace Your Exams
💎
Always Check ALL FOUR LIMB BPs
Upper limb hypertension + lower limb hypotension = CoA until proven otherwise
💡
Pre vs Post-ductal SpO₂
Difference of >3% between right hand (pre-ductal) and foot (post-ductal) = significant right-to-left shunting at PDA level
💎
Don't Give High O₂ in Duct-Dependent Systemic Lesions
O₂ is a potent ductal constrictor. Can worsen CoA/HLHS by closing the PDA
💡
Radio-femoral Delay
Classic clinical sign of CoA. Feel radial and femoral pulse simultaneously — delay in femoral = CoA
💎
Rib Notching — Only in Older Children
Appears after age 5-6 years due to collateral vessels eroding rib undersurfaces. NOT seen in neonates/infants
💡
HLHS = Worst Duct-Dependent Lesion
Single ventricle physiology. Requires Norwood procedure in 3 staged surgeries. High mortality.
💎
VSD — Murmur Appears After Week 1
As pulmonary vascular resistance falls, L→R shunt increases and murmur becomes audible. Not always heard at birth!
💡
Eisenmenger Syndrome — Point of No Return
Uncorrected L→R shunt → pulmonary hypertension → reversal to R→L → inoperable. Early surgery prevents this.
Exam Preparation
High-Yield Points for MD/DNB Paediatrics
Must-Know Facts
Important Associations
ECG & CXR Findings
🎯 In exams: Always correlate ANATOMY → PHYSIOLOGY → CLINICAL FEATURES → INVESTIGATIONS → MANAGEMENT
Viva Questions — Be Ready!
Frequently Asked in MD/DNB/MRCPCH Viva Examinations
Q1: What is the most common site of coarctation?
Juxtaductal — just distal to origin of left subclavian artery, at the level of ductus arteriosus
Q2: How will you clinically diagnose CoA at bedside?
Radio-femoral delay + upper limb hypertension + absent/weak femoral pulses + 4-limb BP difference >10 mmHg
Q3: What is the emergency treatment for a neonate in shock with suspected CoA?
Prostaglandin E1 (0.05-0.1 mcg/kg/min IV) to reopen PDA + supportive care + urgent cardiac referral
Q4: Why should you NOT give high-flow oxygen in a neonate with duct-dependent CoA?
Oxygen causes ductal constriction, closing the PDA which is the only source of lower body blood flow — this will worsen shock
Q5: What CHD is associated with Turner syndrome?
Coarctation of Aorta (most common), also Bicuspid Aortic Valve
Q6: What is Eisenmenger syndrome and when does it occur?
Reversal of left-to-right shunt to right-to-left due to severe pulmonary hypertension from uncorrected large L→R shunt. Lesion becomes inoperable.
Q7: What is the surgical treatment of choice for CoA in a neonate?
Resection with extended end-to-end anastomosis via left posterolateral thoracotomy
Q8: What is the significance of pre vs post-ductal SpO2 difference?
Difference >3% suggests right-to-left shunt at PDA level — seen in duct-dependent systemic lesions
CLOSING STATEMENT
"Every baby born with a heart defect deserves a fighting chance."
Congenital heart disease is not a death sentence — it is a challenge we are fully equipped to meet. As paediatricians and neonatologists, we are often the FIRST and most CRITICAL link in the chain of survival. Knowing when to suspect, when to act, and when to refer is all it takes to give a child their entire lifetime.
✅ Check femoral pulses in EVERY newborn
✅ Know your duct-dependent lesions
✅ Keep PGE1 stocked and ready
✅ Refer early — Don't wait for deterioration
Dr. Ajinkya Kale | MBBS, MD Paediatrics | Neonatal Fellow (UK) | Lactation Consultant (BPNI, AIIMS Nagpur)
Thank You | Questions Welcome 🙏
- pediatric-cardiology
- congenital-heart-disease
- coarctation-of-aorta
- neonatology
- medical-education
- pge1
- acyanotic-chd