
MRKH Syndrome: Uterovaginal Aplasia & Ovarian Function
Explore clinical findings, embryology, and management of Müllerian agenesis (MRKH), including primary amenorrhea diagnosis and neovagina creation methods.
Clinical Overview: Müllerian Agenesis Spectrum
Anatomical Findings, Physiology, and Genetic Profile
Department of Reproductive Endocrinology & Infertility
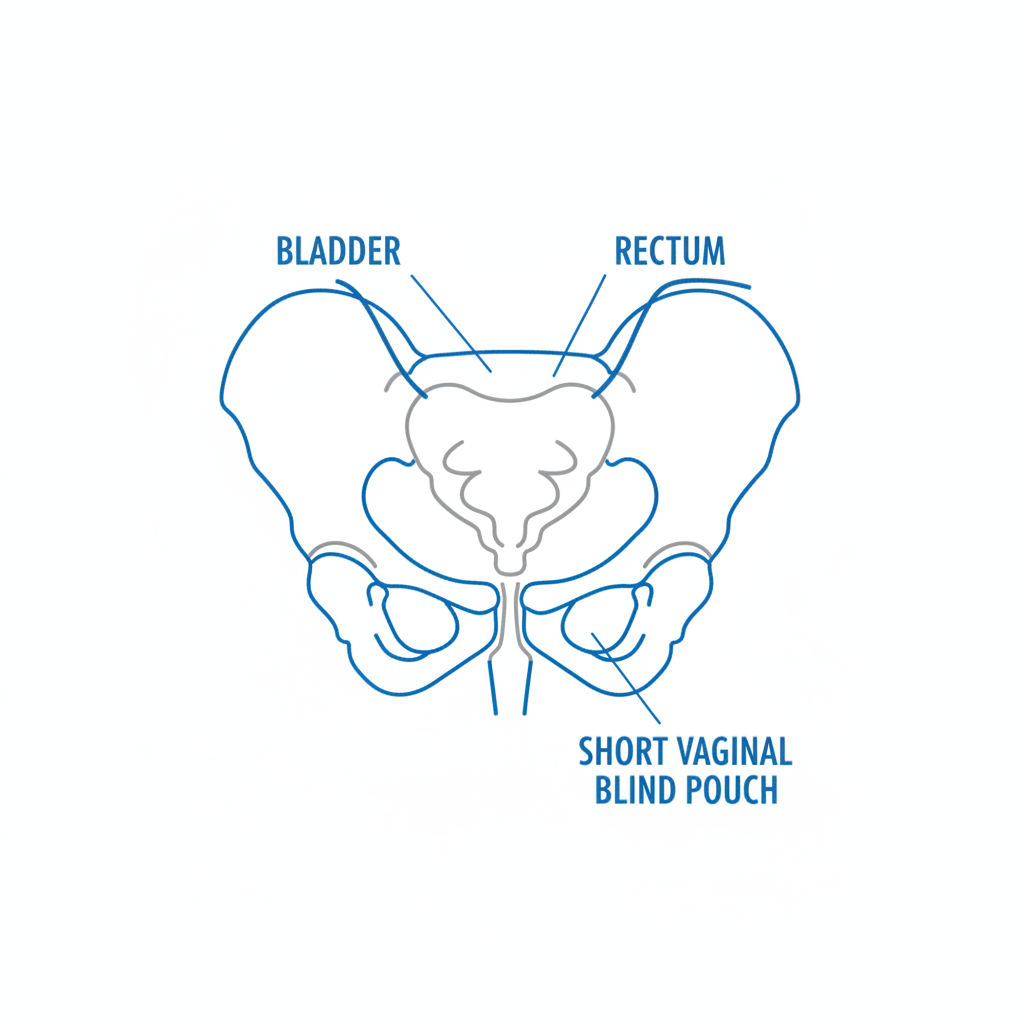
Anatomical Defect: Uterine & Vaginal Aplasia
Primary Finding: Complete absence of the uterus and cervix (Uterine Aplasia).
Vaginal Finding: Absence of the upper 2/3 of the vagina, presenting as a shortened vaginal pouch (2-4 cm deep).
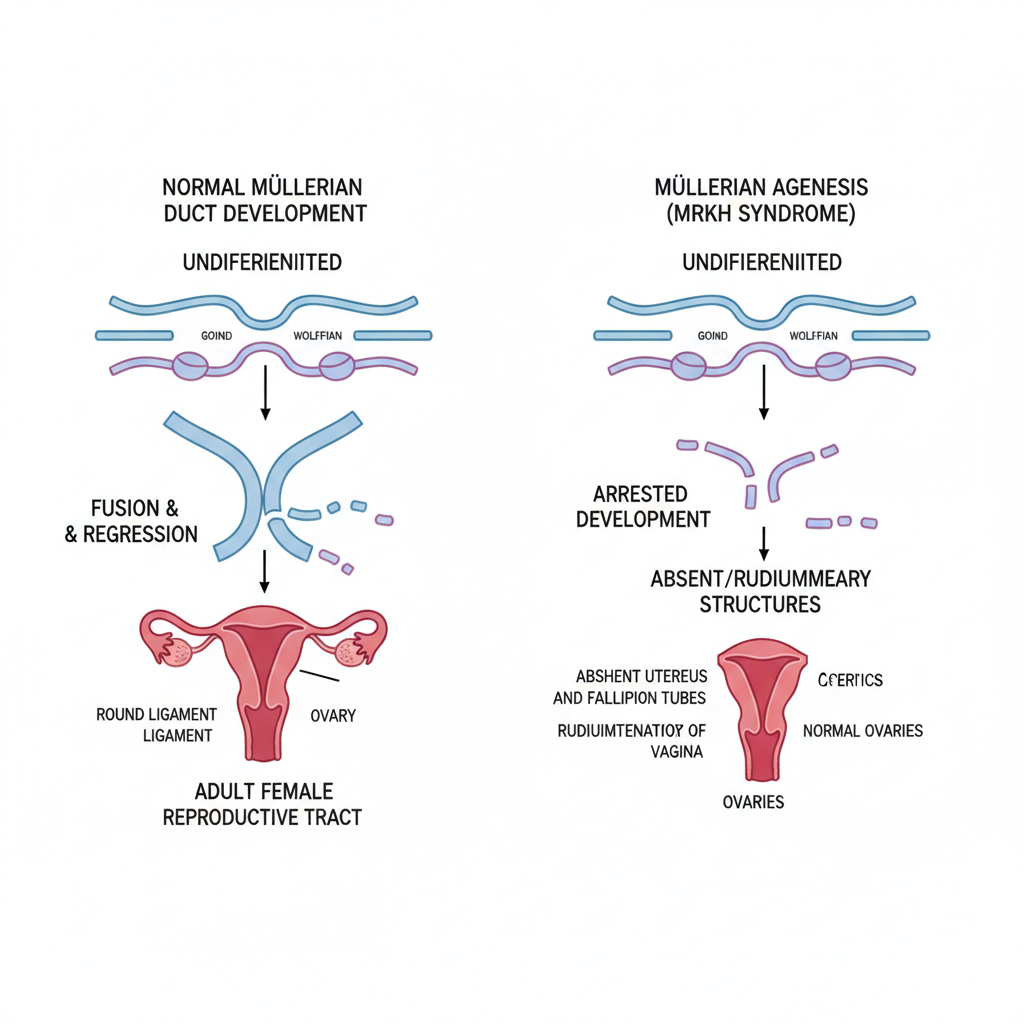
Etiology: Failure of the Müllerian ducts to fuse and develop during embryogenesis.
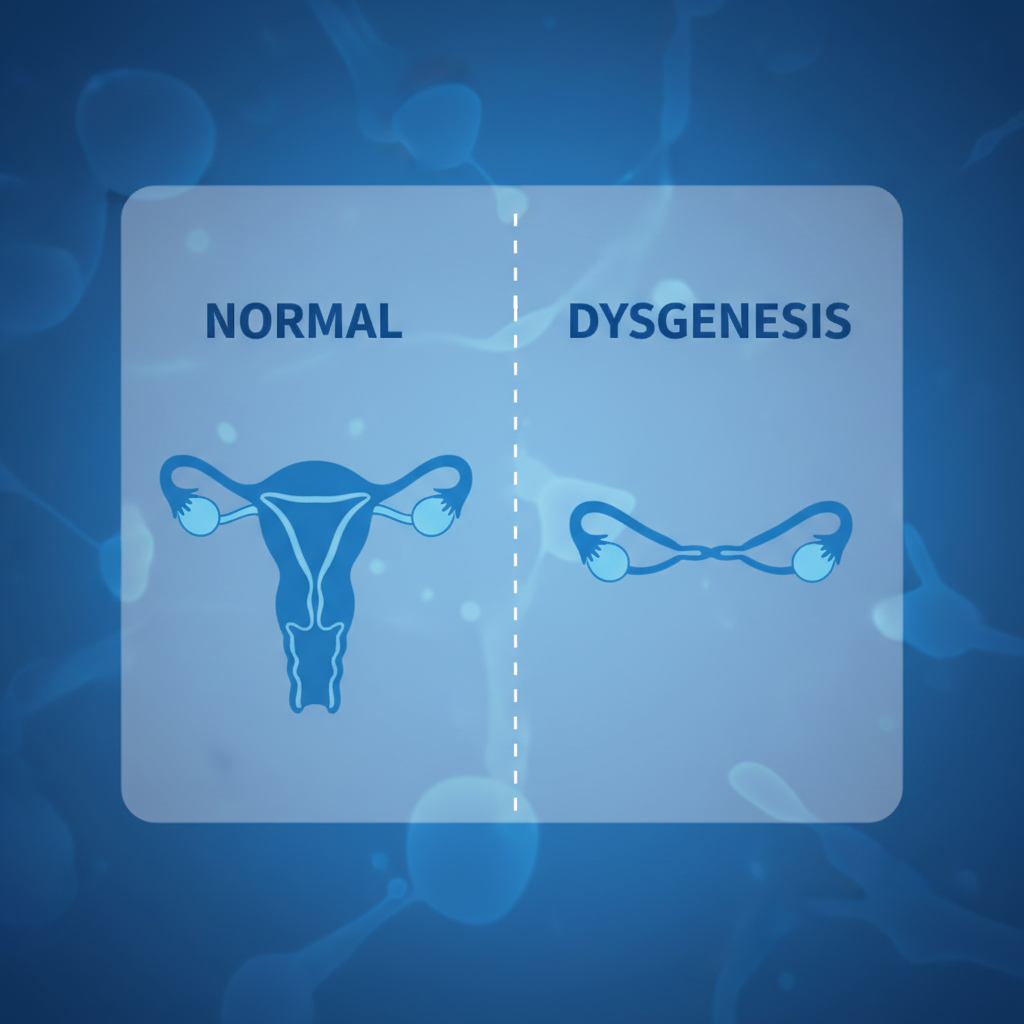
Embryology: Müllerian Dysgenesis
Developmental Arrest: Interruption occurs approx. 7 weeks of gestation.
Mechanism: Failure of the paired Müllerian (paramesonephric) ducts to fuse, canalize, and develop into the uterus/cervix.
Outcome: Formation of rudimentary uterine horns (cornua) connected by a fibrous band, or complete absence.
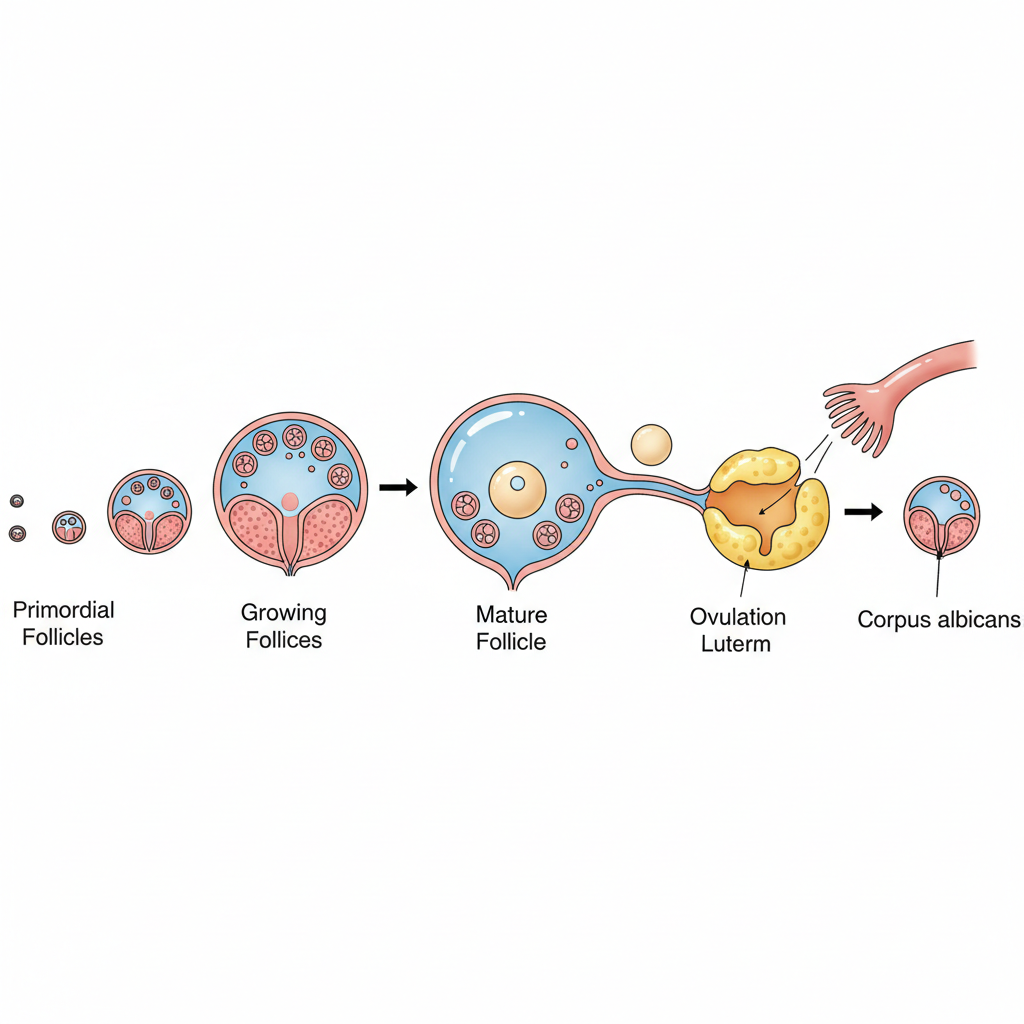
Physiology: Normal Ovarian Function
Despite uterine aplasia, ovaries are embryologically distinct and usually functionally normal.
Normal Folliculogenesis: Recruitment and maturation of follicles occurs cyclically.
Normal Ovulation: Regular release of oocytes confirms functional hypothalamic-pituitary-gonadal axis.
Endocrine Profile: Normal levels of FSH, LH, Estradiol, and Progesterone.
Clinical Exam: Secondary Sexual Characteristics
Patient presents with normal female phenotype appropriate for age.
Breast Development
Normal breast growth (Thelarche) indicating functional estrogen production. Usually Tanner Stage 4 or 5 at presentation.
Pubic/Axillary Hair
Normal hair distribution (Pubarche/Adrenarche) indicating appropriate androgen responsiveness.
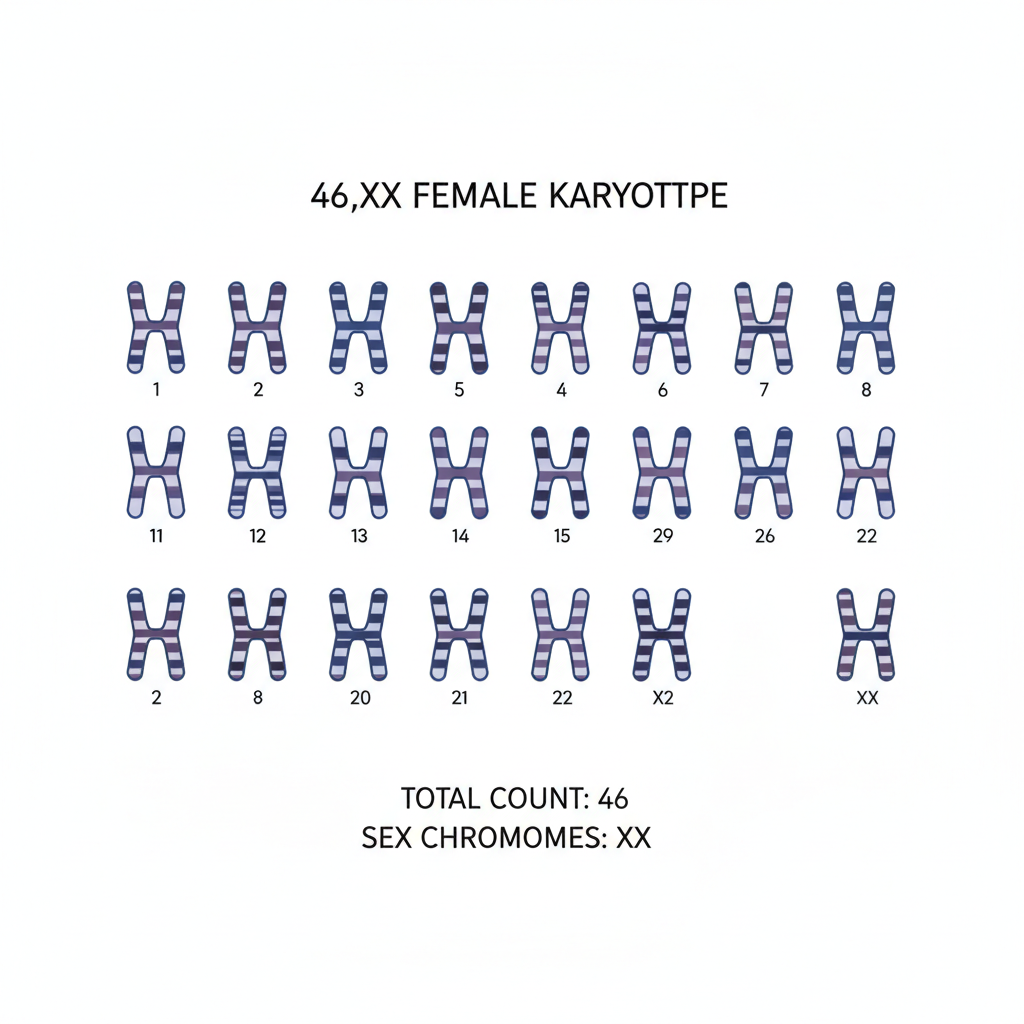
Genetic Profile: Normal Karyotype (46,XX)
Chromosomal Analysis: Distinguishes this condition from Androgen Insensitivity Syndrome (46,XY).
Implication: Genetic sex matches phenotypic sex. Patient is genetically female.
Embryological Basis: Müllerian Agenesis
Mechanism: Dysgenesis of Müllerian ducts (~6 weeks gestation).
Structures Affected: Fallopian tubes, Uterus, Cervix, Upper Vagina.
Structures Spared: Ovaries (primitive yolk sac origin) and Lower Vagina (urogenital sinus origin).
Presentation: Primary Amenorrhea
Incidence
1 in 4,500
Hallmark Sign: Absence of menarche by age 15-16 in an adolescent with normal growth and secondary sexual characteristics.
Coital Difficulty: May present later with inability to engage in vaginal intercourse.
Pain: Cyclic pelvic pain is typically ABSENT unless functional uterine remnants are present (hematometra).
Concomitant Anomalies
Renal: Unilateral renal agenesis, pelvic kidney, horseshoe kidney. Skeletal: Scoliosis, vertebral anomalies (Klippel-Feil).
Differential Diagnosis Checklist
Müllerian Agenesis (MRKH)
46,XX
Normal Female Range
Normal
Androgen Insensitivity (AIS)
46,XY
High Testosterone (Male range)
Sparse / Absent
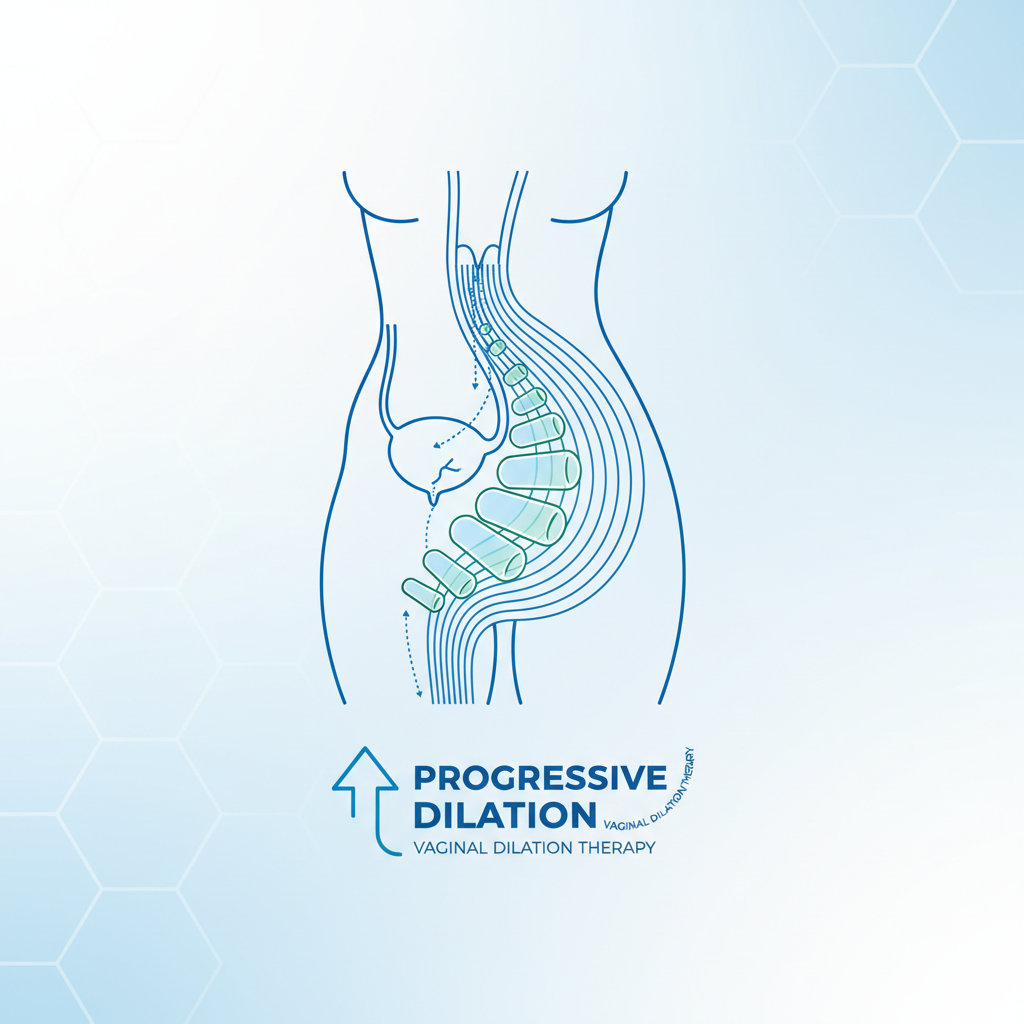
Management: Neovagina Creation
First Line: Dilator Therapy (Frank's Method)
Progressive non-surgical dilation of the vaginal dimple. High success rate (>90%) with compliance.
Second Line: Surgical Vaginoplasty
McIndoe procedure (skin graft), Bowel vaginoplasty, or Vecchietti procedure. Reserved for failure of dilation.
- mrkh-syndrome
- mullerian-agenesis
- reproductive-endocrinology
- primary-amenorrhea
- gynecology
- embryology
- karyotype-46xx