




Necrotizing Enterocolitis (NEC) Management & Guidelines
Comprehensive guide on NEC pathophysiology, Bell's staging, and Waikato Neonatal Medicine management protocols including the STOP bundle and antibiotics.
Necrotizing Enterocolitis (NEC)
Evaluation and Mangement Guidelines for New RMOs in Waikato Neonatal Medicine
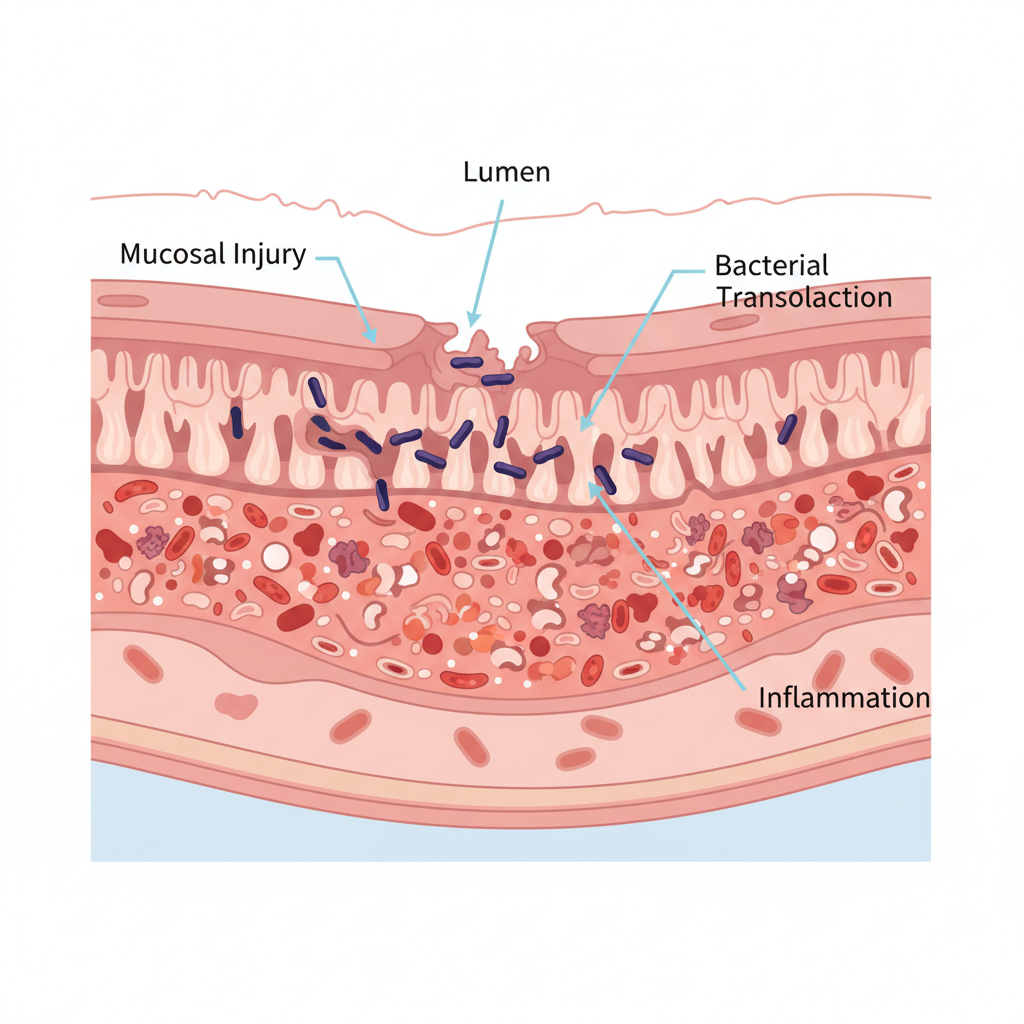
Pathophysiology: The "Double Hit"
• <strong>The Mechanism:</strong> Ischemic, toxic, or inflammatory injury to an immature gut.<br>• <strong>Mucosal Injury:</strong> Disruption of the gut barrier allows bacterial translocation.<br>• <strong>The Inflammatory Cascade:</strong> Release of cytokines (TNF-a, PAF) leads to further necrosis.<br>• <strong>Key Drivers:</strong> Antibiotic dysbiosis, formula feeding, and circulatory instability (hypotension/PDA).
Risk Factors & Epidemiology
• <strong>Prematurity:</strong> >90% of cases occur in VLBW infants.<br>• <strong>Diet:</strong> Formula feeding increases risk significantly compared to breast milk.<br>• <strong>Ischemia:</strong> Perinatal asphyxia or PDA can compromise gut blood flow.<br>• <strong>Timing:</strong> Typically presents 2-3 weeks after birth (inverse relationship to gestational age).
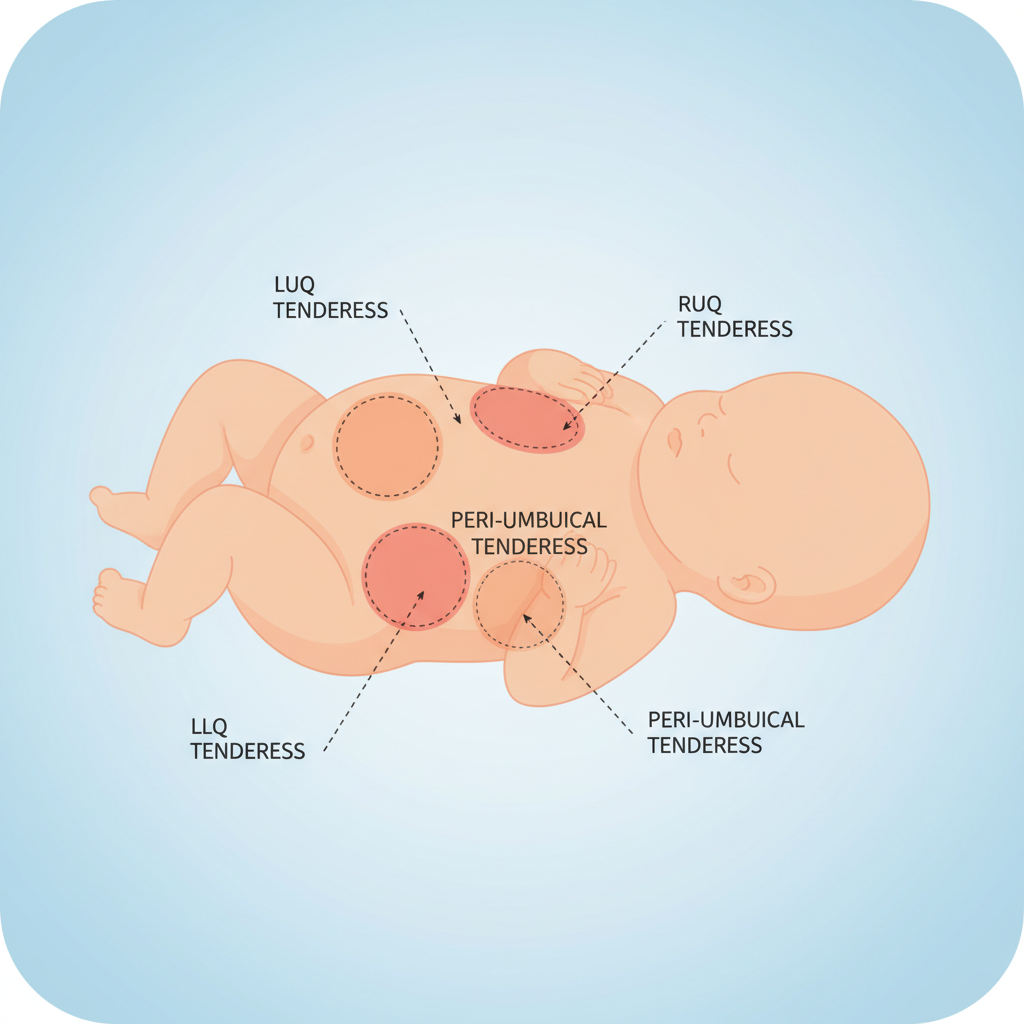
Clinical Presentation: The "Look"
• Temperature instability<br>• Apnea and Bradycardia<br>• Lethargy / Hypoactivity<br>• Hypotension / Shock<br>• Metabolic Acidosis
• Abdominal Distension (measure girth!)<br>• High Gastric Residuals<br>• Bloody Stools<br>• Abdominal Tenderness / Discoloration<br>• Absent Bowel Sounds
Differential Diagnosis & Decision Pathway
<div style="display:grid; grid-template-columns: 1fr 1fr 1fr 1fr; gap:20px; text-align:left;"> <div style="background:#eef6fc; padding:20px; border-top:5px solid #003366;"> <h3 style="color:#003366;">NEC</h3> <p>Pneumatosis, Bloody stool, Systemic illness.</p> </div> <div style="background:#fff0f0; padding:20px; border-top:5px solid #c0392b;"> <h3 style="color:#c0392b;">SIP</h3> <p>Spontaneous Perforation. Focal air, clinically 'well' baby, bluish abdomen.</p> </div> <div style="background:#fef9e7; padding:20px; border-top:5px solid #f1c40f;"> <h3 style="color:#d4ac0d;">Sepsis</h3> <p>Systemic signs (ileus) without pneumatosis. Culture positive.</p> </div> <div style="background:#e8daef; padding:20px; border-top:5px solid #8e44ad;"> <h3 style="color:#8e44ad;">Volvulus</h3> <p>Bilious vomiting, acute onset, surgical emergency (whirlpool sign).</p> </div> </div>
Modified Bell's Staging Criteria
<strong>Stage I (Suspected):</strong><br>• Temperature instability, apnea, lethargy.<br>• Gastric residuals, occult blood.<br>• Normal or mild ileus on X-ray.
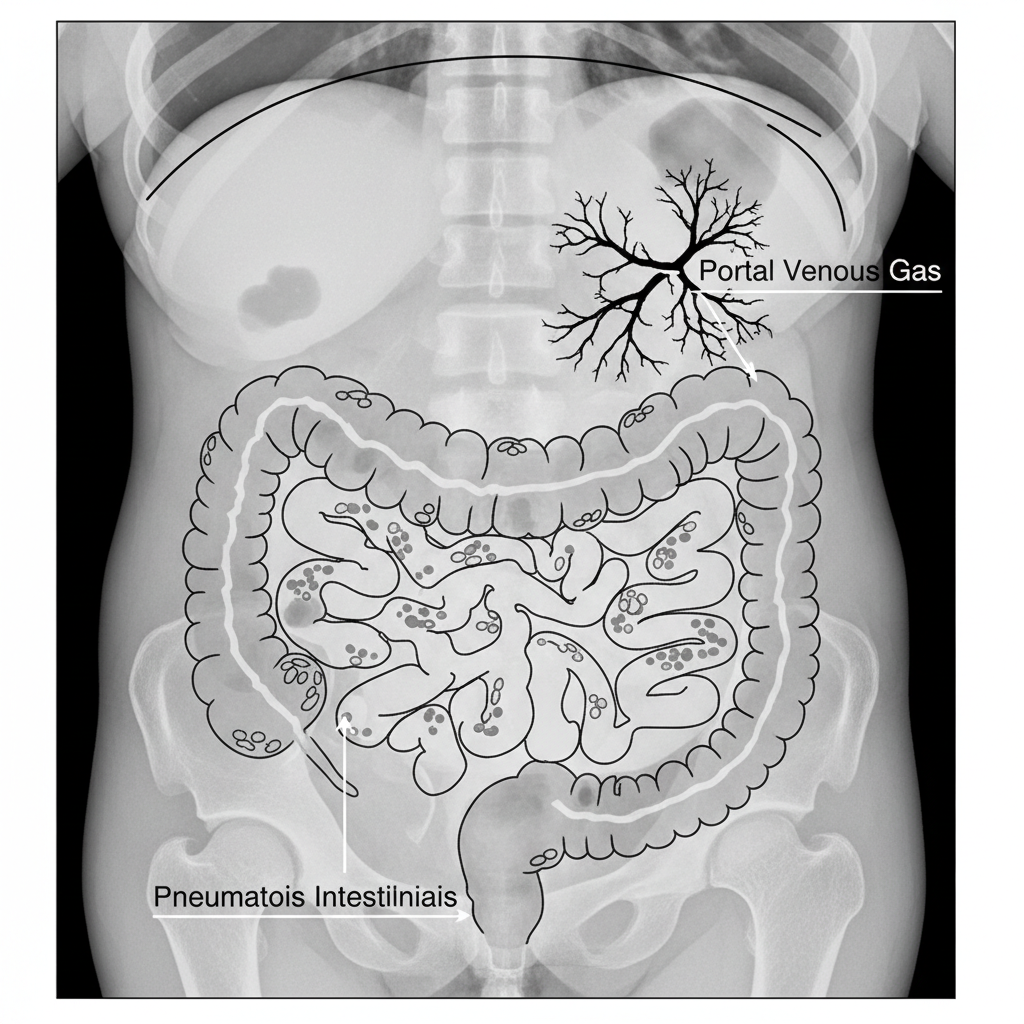
<strong>Stage II (Definite):</strong><br>• Gross bloody stools.<br>• Abdominal tenderness, thrombocytopenia.<br>• X-ray: <strong>Pneumatosis intestinalis</strong>, Portal venous gas.
<strong>Stage III (Advanced):</strong><br>• Hypotension, acidosis, DIC, neutropenia.<br>• Marked distension, peritonitis.<br>• X-ray: <strong>Pneumoperitoneum</strong> (perforation).
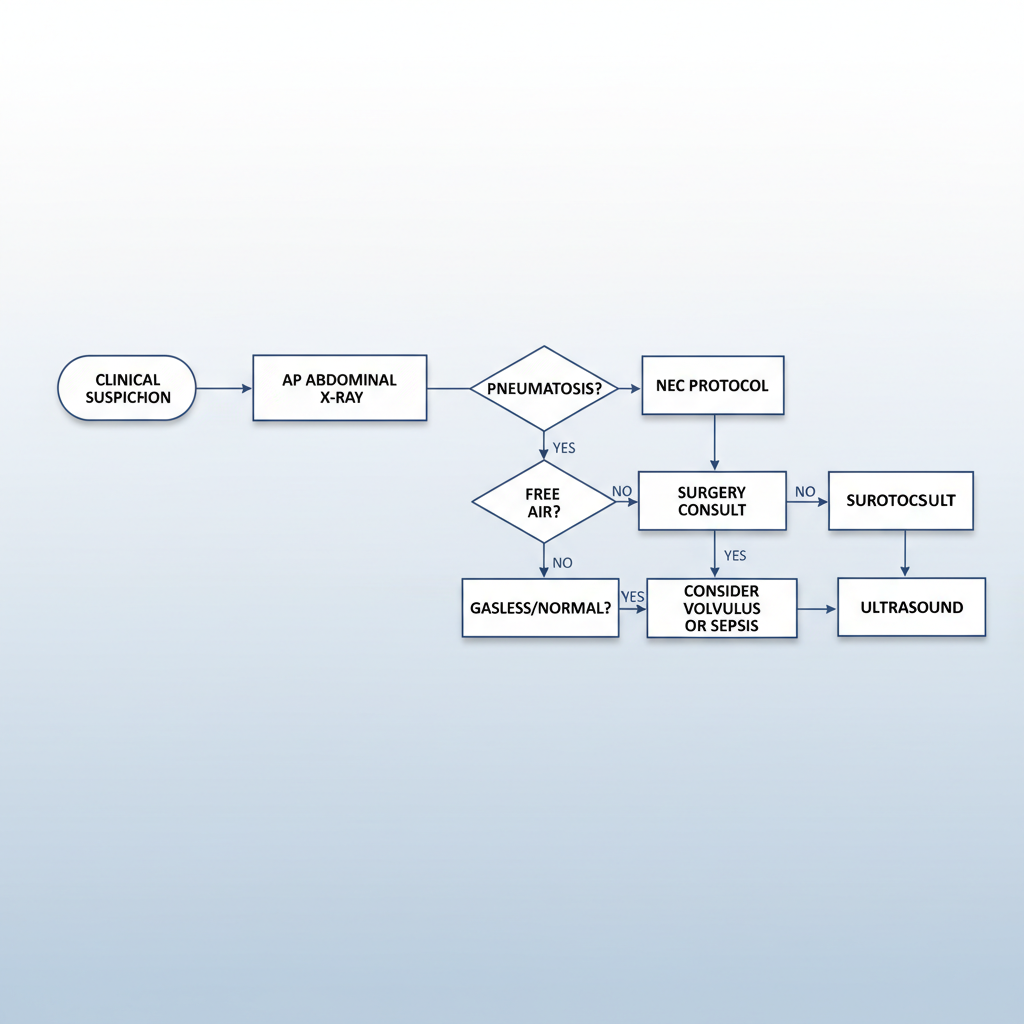
Diagnostics & Imaging Schedule
• <strong>Schedule:</strong> Serial AP AXR every 6-8 hours in acute phase (Stage I/II).<br>• <strong>Key Sign 1:</strong> Pneumatosis Intestinalis (air in bowel wall - bubbles/tracks).<br>• <strong>Key Sign 2:</strong> Portal Venous Gas (branching air over liver).<br>• <strong>Key Sign 3:</strong> Pneumoperitoneum (Rigler's sign / Football sign).<br>• <strong>Ultrasound:</strong> Recommended for early detection or complex fluid collections.
• Full Blood Count (Thrombocytopenia is a bad prognostic sign)<br>• Blood Gas (Metabolic Acidosis, Lactate)<br>• CRP (Trending)<br>• Blood Culture (Pre-antibiotics)<br>• Coagulation Screen (if severe/DIC)
Initial Management: The "STOP" Bundle
<ol> <li><strong>STOP Feeds (NPO):</strong> Bowel rest is critical. Start IV fluids / TPN.</li> <li><strong>Decompression:</strong> Insert large bore NG/OG tube on free drainage. Monitor output.</li> <li><strong>Cultures:</strong> Blood (and CSF/Urine if clinically indicated) *before* antibiotics.</li> <li><strong>Antibiotics:</strong> Immediate initiation (see protocol).</li> <li><strong>Resuscitation:</strong> Fluid bolus (10-20ml/kg) for hypotension/poor perfusion.</li> <li><strong>Pain Control:</strong> Avoid opioids if possible (slows gut), but treat pain (Morphine/Fentanyl) if severe/ventilated.</li> </ol>
Antibiotic Regimen (Waikato Guidelines)
Standard Empiric Therapy:<br><strong>Ampicillin + Gentamicin</strong>
If NEC is Suspected/Confirmed:<br><strong>Add Amoxicillin-Clavulanic Acid</strong>
If Perforation / Surgical NEC:<br><strong>Add Metronidazole</strong> (for anaerobic coverage)<br><em>Consider Vancomycin if MRSA/CONS concern.</em>
<strong>Target Pathogens:</strong><br>• GBS, E. coli, Klebsiella (Early)<br>• Pseudomonas, CONS, Staph Aureus (Late)<br>• Anaerobes (Bacteroides) if perforated.
Escalation & Surgical Management
<strong>Absolute Indications for Surgery:</strong><br>• Pneumoperitoneum (Perforation)<br><br><strong>Relative Indications (Surgical Consult):</strong><br>• Clinical deterioration despite maximal medical capability<br>• Portal venous gas (controversial, but warrants consult)<br>• Persistent fixed loop on X-ray<br>• Abdominal mass / Erythema of abdominal wall
<strong>Transfer Protocol:</strong><br>• Consult Paediatric Surgical Team early.<br>• Secure IV access (central preferred) and airway.<br>• Decompress stomach before transport.<br>• Update parents and document decision time.
Prevention & Long Term Outcomes
• <strong>Breast Milk (EBM):</strong> The #1 protective factor. Donor milk if maternal unavailable.<br>• <strong>Probiotics:</strong> Routinely used in VLBW infants (Waikato protocol).<br>• <strong>Standardized Feeding:</strong> Slow advancement protocols.<br>• <strong>Antibiotic Stewardship:</strong> Limit early empirical use (48h rule).
• <strong>Strictures:</strong> 10-20% of medical NEC survivors. Watch for obstruction later.<br>• <strong>Short Bowel Syndrome:</strong> If extensive resection required.<br>• <strong>Neurodevelopment:</strong> NEC is an independent risk factor for poor neurodevelopmental outcomes.
- necrotizing-enterocolitis
- neonatal-medicine
- pediatrics
- medical-guidelines
- nicu
- bell-staging
- pathophysiology