
Postpartum Hemorrhage Management: Clinical Protocols
Expert guide on PPH management: ACOG definitions, the 4 T's of etiology, Shock Index thresholds, uterotonics, TXA dosage, and surgical escalation steps.
Postpartum Hemorrhage Management
Clinical Protocols, Recognition, and Emergency Response
Defining PPH: ACOG vs. WHO
Cumulative blood loss ≥ 1,000 mL OR blood loss accompanied by signs/symptoms of hypovolemia within 24 hours after the birth process.
Traditional definition: ≥ 500 mL (vaginal) or ≥ 1,000 mL (cesarean). New emphasis on clinical instability.
Etiology: The 4 T's Frequency
Uterine Atony (Tone) accounts for 70-80% of all PPH cases.
Recognition: Quantitative Blood Loss (QBL)
Visual estimation underestimates loss by 30-50%.
Protocol: Weigh all blood-soaked materials (1g = 1mL).
Keep a running total displayed on the whiteboard.
The Shock Index (SI) as Early Warning
SI = Heart Rate ÷ Systolic BP. Normal range is 0.5-0.7 for non-pregnant, 0.7-0.9 for pregnant.
First-Line Medical Management: Uterotonics
OXYTOCIN
First Line. 10-40 units IV infusion (or IM). No contraindications.
METHYLERGONOVINE
0.2 mg IM q2-4hr. AVOID in Hypertension/Preeclampsia.
CARBOPROST (Hemabate)
250 mcg IM q15-90min. AVOID in Asthma.
MISOPROSTOL
800-1000 mcg Rectal. Safe in HTN/Asthma. Slow onset.
Tranexamic Acid (TXA)
TIMING IS CRITICAL: Administer within 3 hours of birth.
Dose: 1 gram IV over 10 minutes.
Mechanism: Antifibrinolytic (Prevents clot breakdown).
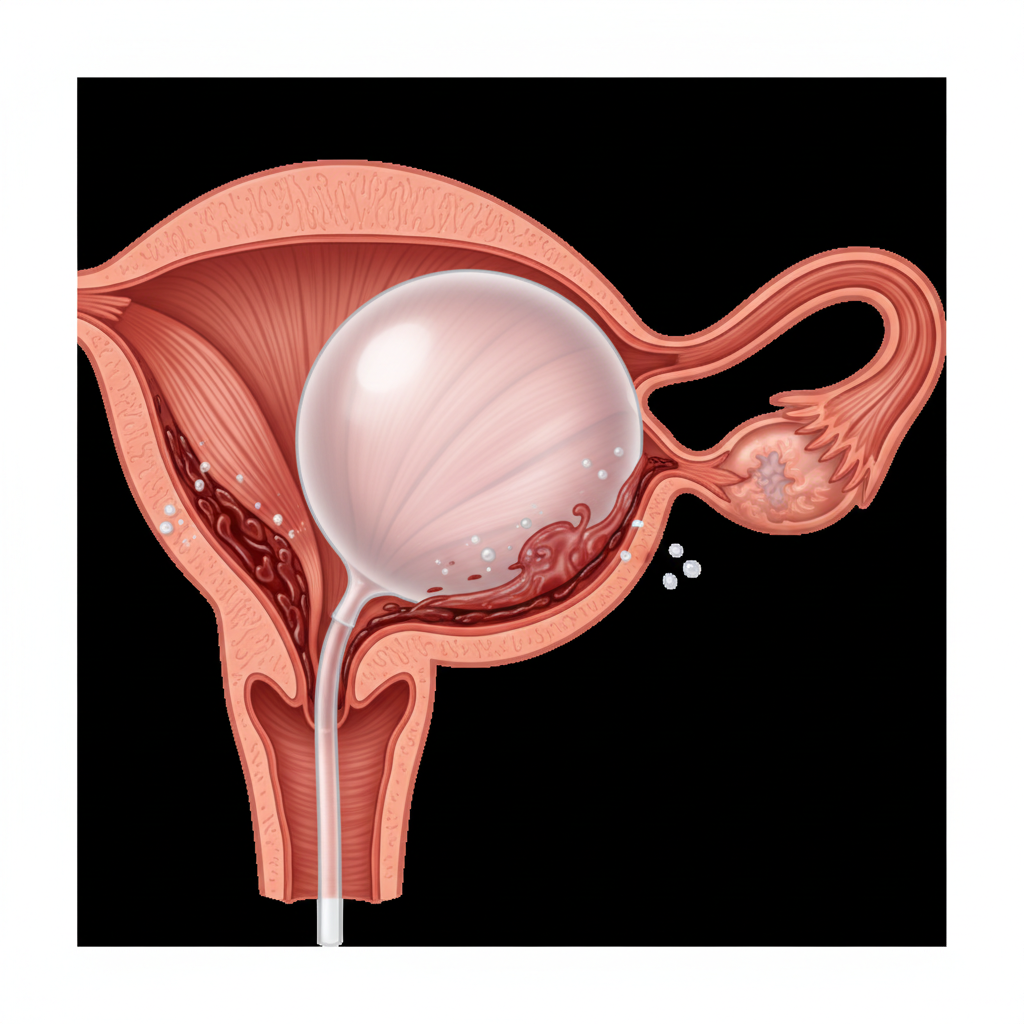
Intrauterine Balloon Tamponade (UBT)
When Uterotonics Fail
1. Inflate with 300-500mL sterile saline.<br>2. Can be combined with compression sutures (sandwich).<br>3. Monitor drainage output continuously.
Massive Transfusion Protocol (MTP)
Orchestrated Release ratio 1:1:1
TRIGGER: >1500mL QBL, VS instability, or ongoing bleeding.
Surgical Escalation Ladder
1. Uterine Conservation
D&C, Compression Sutures (B-Lynch).
2. Vascular Ligation
Uterine Artery, Ovarian Artery, Internal Iliac (Hypogastric).
3. Hysterectomy
Definitive management when all else fails.
Summary: PPH Algorithm
STAGE 1: Activate > Fundal Massage > Oxytocin > Empty Bladder > TXA > 2nd Line Meds
STAGE 2: Move to OR > Balloon Tamponade (UBT) > Consider MTP
STAGE 3: Surgical Intervention > MTP > Hysterectomy
- postpartum-hemorrhage
- obstetrics
- emergency-medicine
- clinical-protocols
- maternal-health
- pph-algorithm
- medical-education