


2025 ESC/EACTS Valvular Heart Disease Guidelines Summary
Explore the 2025 ESC/EACTS updates on Valvular Heart Disease, featuring new TAVI age thresholds, TEER recommendations, and multimodality imaging protocols.
ESC/EACTS 2025 GUIDELINES
Valvular Heart
Disease
Management Guidelines — Key Recommendations & Updates
Published August 2025
Heart Team Approach
Updated Evidence-Based
European Society of Cardiology (ESC) & European Association for Cardio-Thoracic Surgery (EACTS)
Presentation Outline
01
Introduction & Overview
02
Heart Team & Heart Valve Centres
03
Diagnostic Advances & Imaging
04
Aortic Stenosis (AS)
05
Aortic Regurgitation (AR)
06
Mitral Regurgitation (MR)
07
Tricuspid Valve Disease
08
Prosthetic Valves & Antithrombotic Management
Introduction & Scope of the 2025 Guidelines
<b style="color: #FFFFFF;">Published:</b> August 29, 2025 — Update to the 2021 ESC/EACTS VHD Guidelines
<b style="color: #FFFFFF;">Covers:</b> Acquired valvular heart disease in adults
Integrates new RCT evidence on TAVI, TEER, and transcatheter tricuspid interventions
Emphasis on patient-centered, lifetime management strategies
Endorsed by multiple national cardiac societies worldwide
The right intervention, for the right patient, at the right time — by the right team.
8
Major Valvular Conditions Covered
100+
New Evidence-Based Recommendations
2021 → 2025
Major Updates Incorporated
Heart Team & Heart Valve Centres
Class I Recommendation
Core Heart Team Members
🫀
Imaging Cardiologist
⚕️
Interventional Cardiologist
🔪
Cardiac Surgeon
Extended Team Members
Heart Failure Specialist
Geriatrician
Anesthesiologist
Neurologist / Stroke Team
Heart Valve Centres must perform ≥100 valve procedures/year
(≥50 TAVI · ≥25 SAVR)
📊
High Volume = Better Outcomes
Volume-outcome data supports referral for complex procedures
🌐
Multidisciplinary Networks
Triage patients from surveillance clinics to intervention centres
🛡️
Reduces Undertreatment
Systematic approach improves diagnosis and treatment rates
Diagnostic Advances & Multimodality Imaging
Multimodality imaging is central to precise VHD assessment, staging, and procedural planning.
ECHOCARDIOGRAPHY
3D Echo for precise anatomy
Vena contracta area for MR/TR
Exercise stress echo for dynamic assessment
Pitfalls in mixed/multivalvular disease
ADVANCED IMAGING
Cardiac CT (CCTA): Class I for low-moderate CAD risk pre-intervention
CMR for myocardial fibrosis & function
3D printing for procedural planning
CT for TAVI sizing & access planning
BIOMARKERS & TESTS
NT-proBNP for risk stratification
Exercise testing for asymptomatic patients
6-minute walk test
Frailty assessment tools
CCTA now Class I recommendation before valve interventions in patients with moderate or lower pretest likelihood of CAD (Level of Evidence B)
Aortic Stenosis
Key 2025 Recommendations
Age Cutoff Lowered
TAVI preferred ≥70 yrs (was ≥75 yrs)
Early Intervention
Asymptomatic severe AS: Class IIa for low-risk (LVEF >50%)
TAVI PREFERRED
Age ≥70 years
High/intermediate surgical risk
Tricuspid aortic valve
Limited life expectancy
Frailty / comorbidities
SAVR PREFERRED
Age <70 years
Young, low-risk patients
Bicuspid aortic valve / root disease
Long life expectancy / durability needed
Good surgical candidate
Class I
Symptomatic severe AS → Intervention indicated
Class IIa
Asymptomatic severe high-gradient AS, low-risk, LVEF >50%
Class IIb
TAVI for bicuspid AS or high-risk aortic regurgitation
Aortic Regurgitation — Management Updates
SURGICAL INDICATIONS (Class I)
Symptomatic severe AR
Asymptomatic severe AR with LVEF ≤50%
Asymptomatic severe AR with LVESD >50mm or LVEDD >70mm
Severe AR undergoing other cardiac surgery
NEW 2025 UPDATE
Class IIb: TAVI may be considered for severe AR in patients ineligible for surgery (Level B)
MEDICAL MANAGEMENT
Vasodilators (ACE inhibitors/ARBs) for symptomatic patients
Beta-blockers for Marfan/aortopathy patients
Regular surveillance imaging (echo every 1–2 years for moderate AR)
Mild
Moderate
Severe
LVEF ≤50% or LVESD >50mm
Aortic root/ascending aorta intervention thresholds remain at ≥55mm (≥50mm for Marfan/bicuspid)
Mitral Regurgitation — Primary & Secondary MR
Primary (Degenerative) MR
Class I Surgery Indications:
Symptomatic severe primary MR
Asymptomatic severe MR with LVEF 60–70% or LVESD 40–45mm
Asymptomatic severe MR + new AF or pulmonary hypertension
Repair preferred over replacement. Minimally invasive approaches endorsed.
Repair rate >90% at experienced centres
Secondary (Functional) MR
Ventricular SMR:
Class I: TEER (MitraClip/PASCAL) if COAPT criteria met (ERO ≥0.3 cm²) after optimized GDMT
Reduces HF hospitalizations significantly
Atrial SMR:
Class IIa: Surgery or TEER if symptomatic despite GDMT
Address underlying AF and left atrial dilation
TEER upgraded to Class I for ventricular secondary MR meeting COAPT criteria — after guideline-directed medical therapy optimization
Tricuspid Valve Disease — Updated Recommendations
2025 Upgrades at a Glance
Concomitant TR Repair: Class I
Isolated TR Surgery: Class IIa
Transcatheter TEER for TR: Class IIa
Indications for TR Intervention
Class I
Concomitant tricuspid repair during left-sided valve surgery (even for moderate TR if progressive)
Severe symptomatic TR after left-sided surgery
Class IIa
Isolated severe symptomatic TR despite GDMT → Surgery or transcatheter TEER/replacement
TR with right heart dilation before irreversible RV dysfunction
Transcatheter Tricuspid Options
TEER (edge-to-edge repair) — e.g., TriClip, PASCAL
Transcatheter tricuspid replacement (TTVR)
Bicaval valve implantation for severe TR
Transcatheter options expanding rapidly — RCT evidence growing
Early intervention before irreversible RV dysfunction is critical for improved outcomes
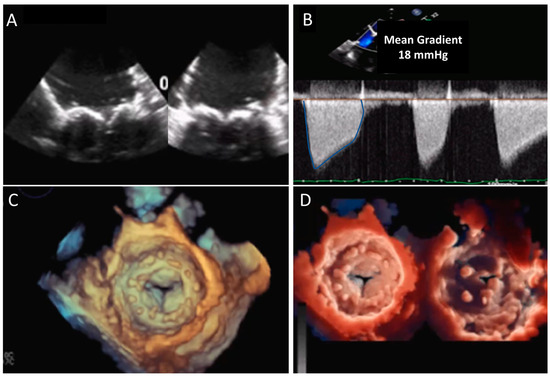
Mitral Stenosis — Rheumatic & Calcific
Rheumatic Mitral Stenosis
MVA ≤ 1.5 cm² = Severe MS
Symptomatic severe MS (MVA ≤ 1.5 cm²)
Asymptomatic severe MS with new-onset AF or pulmonary HTN
Percutaneous Mitral Commissurotomy (PMC) if favorable anatomy (Wilkins score ≤ 8), no MR, no thrombus
Mitral valve replacement if PMC not suitable
Calcific Mitral Annular Disease
Emerging transcatheter options for MAC-related MS
Higher procedural risk due to calcification
Transcatheter mitral valve replacement (TMVR)
— Class IIb consideration
Careful patient selection with CT planning essential
All patients with MS and AF: Anticoagulation with VKA (not DOACs) — Class I
Asymptomatic MS with AF: Anticoagulation indicated regardless of stroke risk score
Prosthetic Valves & Antithrombotic Therapy
Patient education on anticoagulation self-monitoring is strongly emphasized in 2025 guidelines.
What's New?
2021 → 2025 Key Updates
TAVI Age Threshold
UPDATED
Age cutoff for TAVI preference lowered from <span style="color:#FFFFFF; font-weight:600;">75 → 70 years</span> for tricuspid aortic stenosis
Asymptomatic AS
UPDATED
<span style="color:#FFFFFF; font-weight:600;">Class IIa:</span> Early intervention for asymptomatic severe high-gradient AS in low-risk patients (LVEF >50%) — supported by EARLY TAVR trial
Secondary MR TEER
UPGRADED
TEER upgraded to <span style="color:#FFFFFF; font-weight:600;">Class I</span> for ventricular SMR meeting COAPT criteria after optimized GDMT
Tricuspid Intervention
UPGRADED
Concomitant TR repair: <span style="color:#FFFFFF; font-weight:600;">Class I</span>. Isolated severe TR: <span style="color:#FFFFFF; font-weight:600;">Class IIa</span> for surgery or transcatheter TEER
CCTA Pre-Intervention
NEW
CCTA now <span style="color:#FFFFFF; font-weight:600;">Class I</span> before valve interventions in patients with moderate or lower CAD risk (Level B)
AR Transcatheter
NEW
<span style="color:#FFFFFF; font-weight:600;">Class IIb:</span> TAVI may be considered for inoperable severe aortic regurgitation (Level B)
These updates reflect integration of landmark RCT evidence (EARLY TAVR, COAPT, TRILUMINATE)
Summary & Key Takeaways
2025 Guidelines | European Society of Cardiology
Heart Team approach is mandatory
— multidisciplinary, high-volume centres deliver best outcomes
Earlier intervention thresholds
— asymptomatic patients now benefit from timely treatment
TAVI is preferred ≥70 years for AS;
transcatheter options expanding across all valves
Multimodality imaging (echo, CCTA, CMR)
is essential for diagnosis and procedural planning
Lifetime management perspective
— consider durability, reintervention risk, and patient values
The goal is to deliver the right intervention, to the right patient, at the right time — by the right multidisciplinary team.
- cardiology
- heart-disease
- medical-guidelines
- tavi
- cardiac-surgery
- echocardiography
- healthcare
- esc-guidelines