










Global Mental Health: Discontents and Ways Forward
Explore inequities, innovations, and transformative principles in global mental health, including decolonization, digital health, and task-sharing models.
Two-Hour Academic Lecture | March 2026
Global Mental Health
Discontents & Ways Forward
Exploring Inequities, Innovation, and Transformative Principles in Mental Health Systems Worldwide
Sections: Introduction · Challenges · COVID-19 · Transformation · Policy · Decolonization · Case Studies · Future Directions
SECTION ONE
Introduction to Global Mental Health
Defining the Field · Scale of the Problem · Why It Matters
What Is Global Mental Health?
A field of study, research, and practice that prioritizes improving mental health for all people worldwide — especially in LMICs
Integrates epidemiology, public health, anthropology, psychology, and human rights
Bridges individual care and population-level systems thinking
Emerged formally in the early 2000s; WHO's Mental Health Action Plan (2013–2030) is a landmark framework
Mental, neurological and substance use disorders account for 13% of the global burden of disease
— WHO
Global Burden
Of disease is attributed to mental, neurological, and substance use disorders
Section 1 · Introduction to Global Mental Health
The Scale of the Problem
1 in 8
People worldwide live with a mental disorder (WHO, 2022)
~$1 Trillion
Lost annually in productivity due to depression & anxiety
75%
Of people with mental disorders in LMICs receive NO treatment
70%
Of global mental health resources concentrated in high-income countries
Source: World Health Organization Mental Health Atlas, 2022; Lancet Commission on Global Mental Health
Section 1 · Introduction to Global Mental Health
02
SECTION TWO
Current Challenges & Discontents
Inequities · Stigma · Resource Gaps · Cultural Critiques
Inequities in Access to Care
Treatment gap in LMICs for mental disorders exceeds 75% for most conditions
Only 2% of global health budgets allocated to mental health in low-income countries vs. 5–6% in high-income countries
Psychiatrist density: 0.1 per 100,000 in low-income countries vs. 10+ per 100,000 in high-income countries
Rural and marginalized populations face compounded barriers: cost, distance, language, and discrimination
Fragmented service delivery — mental health siloed from primary and community health care
Low-income countries: 1 psychiatrist per 1 MILLION people
Section 2 · Current Challenges & Discontents
Stigma, Human Rights & Service Failures
Stigma & Discrimination
Social stigma drives delayed care-seeking and self-stigma
Stigma in healthcare settings compounds harm
Media portrayal reinforces negative stereotypes
Human Rights Violations
Involuntary detention and treatment remain widespread
Chaining, restraint, and abuse in psychiatric institutions documented globally
Rights-based frameworks still poorly implemented
Fragmented Systems
Mental health siloed from primary care
Lack of continuity between hospital and community care
Insufficient integration of social services and support
"The treatment gap is not just a resource problem — it is a system design problem."
Section 2 · Current Challenges & Discontents
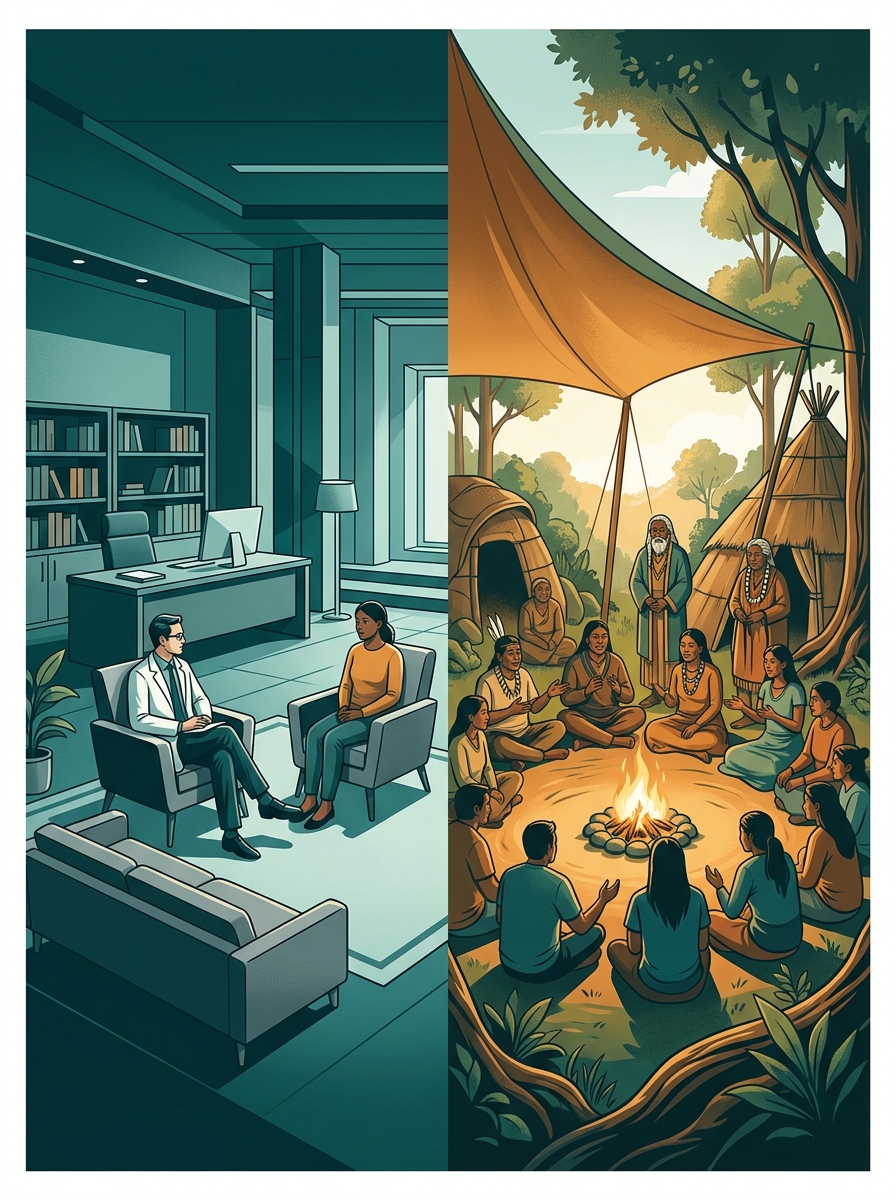
Cultural Critiques of Global Mental Health
Dominant global mental health frameworks are rooted in Western biomedical models — raising important challenges:
DSM and ICD diagnostic categories may not translate cross-culturally — 'category fallacy' (Kleinman, 1987)
Culture-bound syndromes and idioms of distress are often pathologized or ignored
Western 'psy' disciplines exported to LMICs without adaptation — known as 'psychiatric imperialism'
Community-based and traditional healing practices marginalized in formal systems
Research agenda dominated by high-income country institutions — 'helicopter research'
"The universalization of Western categories risks doing more harm than good in culturally distinct contexts."
Section 2 · Current Challenges & Discontents
SECTION THREE
Impact of COVID-19 on Global Mental Health
Escalating Needs · Digital Innovation · Task-Sharing Models
COVID-19: A Global Mental Health Crisis
25%
Increase in global prevalence of anxiety disorders in year 1 of COVID-19 (WHO, 2022)
25%
Increase in depression globally in the same period
93%
Of countries reported disruption to essential mental health services during pandemic
Drivers of Crisis
Lockdowns and social isolation
Bereavement and grief at scale
Economic stress and job losses
Fear, uncertainty, and health anxiety
Disruption to existing care and support systems
Disproportionate Impact On:
Women and caregivers
Young people and adolescents
Healthcare workers (burnout, PTSD)
People with pre-existing mental disorders
Populations in conflict-affected settings
Section 3 · Impact of COVID-19
Innovative Responses to the Crisis
Digital Mental Health Platforms
Rapid scale-up of teletherapy and digital counseling services
Mental health apps (Woebot, Wysa, MindShift) reached millions
Digital tools bridged geography and stigma barriers
Chatbots and AI-assisted screening deployed at scale
Task-Sharing & Community Models
Non-specialist providers (community health workers, peers) trained rapidly
Stepped-care models triaged by severity
WHO mhGAP Intervention Guide accelerated adoption
Lay counselor programs expanded in Sub-Saharan Africa and South Asia
Policy & Systemic Responses
National helplines established or scaled
Mental health integrated into COVID-19 emergency response plans
Funding increased in some countries (UK, Australia)
WHO's MH-COVID platform — global knowledge sharing
The pandemic revealed both the fragility and the adaptability of global mental health systems.
Section 3 · Impact of COVID-19
SECTION FOUR
Principles for System Transformation
Early Action · Dimensional Thinking · Rights-Based Care · Lived Experience
Five Transformative Principles
Address Harmful Social Environments Early in Life
Tackle adverse childhood experiences, poverty, violence, and trauma at their roots — prevention must begin before illness emerges
Adopt a Dimensional Rather Than Categorical Approach
Move beyond rigid diagnostic labels; recognize a spectrum of mental health needs and tailor interventions accordingly
Empower Diverse Frontline Providers
Train and support community health workers, peer specialists, teachers, and primary care workers as mental health providers
Embrace Rights-Based, Non-Coercive Care
Eliminate forced treatment and detention; uphold autonomy, dignity, and informed consent in all mental health settings
Center People with Lived Experience
Ensure those with mental health conditions co-design, co-deliver, and co-evaluate policies and services
Section 4 · Principles for System Transformation
Task-Sharing & Frontline Provider Models
Task-sharing — delegating mental health care to non-specialist providers — is the most scalable solution for LMICs.
Community health workers trained in mhGAP Intervention Guide deliver frontline mental health care
Peer support specialists with lived experience extend reach and reduce stigma
Teachers and school counselors address youth mental health at scale
Primary care integration: mental health embedded in general health consultations
Lay counselors in sub-Saharan Africa demonstrated effectiveness in RCTs (e.g., Friendship Bench, Zimbabwe)
Friendship Bench (Zimbabwe):
500+ lay counselors trained; significant reductions in depression and suicidal ideation
Stepped-Care Cascade
Psychiatrists & Specialists
Primary Care & Nurses
Community Workers, Peers, Lay Counselors
Section 4 · Principles for System Transformation
SECTION FIVE
Policy Recommendations & Implementation Strategies
Whole-of-Society Approaches · Care Redesign · Evidence-Based Investment · Accountability
A Whole-of-Society Approach
Prevention & Promotion
Integrate mental health into education, workplace, and public health policies
Address poverty, discrimination, and adverse childhood experiences systemically
Invest in community resilience and social capital
Care Delivery Redesign
Seamless stepped-care continuum: from community to specialist levels
Deinstitutionalization with robust community alternatives
Integration of mental, physical, and social health services
Evidence & Accountability
Invest in locally-relevant, LMICs-led research
National mental health information systems and monitoring frameworks
Regular reporting against WHO Mental Health Action Plan indicators
Mental Health<br>Policy
Education
Workplace
Health
Housing
Justice
Social Protection
Section 5 · Policy Recommendations
Implementation: From Policy to Practice
PLAN
National mental health strategies aligned to WHO targets
INVEST
Dedicated budgets; public-private partnerships
IMPLEMENT
Scale evidence-based interventions; train workforce
MONITOR
Track outcomes, equity metrics, human rights compliance
Key Implementation Levers
Political will and health ministry leadership
Multi-sectoral coordination mechanisms
Community engagement and co-design
Decentralized service delivery
Common Barriers to Overcome
Siloed government departments
Donor fragmentation and short funding cycles
Insufficient data and evaluation capacity
Workforce shortages and burnout
Section 5 · Policy Recommendations
06
SECTION SIX
Decolonizing Global<br>Mental Health
Power & Knowledge · Global South Perspectives · Mad Studies · Epistemic Justice
The Case for Decolonization
Colonial legacies continue to shape who defines, researches, and treats mental illness globally.
Power Imbalances in Global Mental Health
Research agendas set by high-income country institutions and funders
Global South researchers underrepresented in top journals and conferences
'Helicopter research' — data extracted without local benefit or authorship
Biomedical models promoted over indigenous healing systems
Mad Studies & Service User Movements
Mad Studies challenges medicalization and psychiatric diagnosis as social constructs
Service user/survivor movements demand representation in policy and research
Neurodiversity paradigm: difference, not disorder
Anti-psychiatry critiques: Szasz, Foucault, and their contemporary relevance
Section 6 · Decolonizing Global Mental Health
Toward Epistemic Justice in Mental Health
Pluralism of Knowledge Systems
Recognize and integrate traditional, spiritual, and indigenous healing frameworks alongside biomedical approaches; avoid hierarchy of knowledge
Co-Production & Lived Experience Leadership
People with lived experience of mental illness must co-design, co-research, and co-lead mental health systems — not just as 'service users' but as experts
Equitable Research Partnerships
North-South partnerships must be truly equitable: shared authorship, local IRB leadership, capacity-building, and knowledge returned to communities
"Decolonizing global mental health is not about rejecting science — it is about expanding whose science counts."
Section 6 · Decolonizing Global Mental Health
SECTION SEVEN
Case Studies & Examples
Zimbabwe · India · Australia · Uganda · Brazil
LMIC INNOVATION
Case Study: The Friendship Bench — Zimbabwe
What Is It?
Community mental health intervention delivered by trained older women ('grandmothers') as lay counselors
Wooden bench placed outside primary healthcare clinics — accessible, non-stigmatizing
Evidence-based problem-solving therapy (PST) adapted for local context
Founded by Dr. Dixon Chibanda
Evidence & Impact
Randomized controlled trial (2016, JAMA): Significant reduction in depression and suicidal ideation vs. control
Scaled to 70+ clinics across Zimbabwe; replicated in NYC, Malawi, Kenya
Serves 30,000+ people annually
Low cost: ~$15 per person per year
Key Lessons
Cultural adaptation and trust-building are critical to effectiveness
Lay counselors can deliver high-quality evidence-based care
Community integration reduces stigma
Section 7 · Case Studies
Case Studies: India & Australia
SOUTH ASIA
NIMHANS Community Mental Health — India
India's mental health treatment gap: ~80–85%
HIGH-INCOME COUNTRY
Headspace — Australia
50% of mental disorders begin before age 14
Section 7 · Case Studies
Case Studies: Uganda & Brazil
SUB-SAHARAN AFRICA
BasicNeeds Uganda — Community Mental Health
Uganda: 1 psychiatrist per 1.5 million people
LATIN AMERICA
Psychosocial Care Centres (CAPS) — Brazil
Brazil closed 70%+ of psychiatric beds since 1990 reform
Section 7 · Case Studies
08
SECTION EIGHT
Future Directions
Digital Innovation · Climate & Mental Health · Equity Agenda · Research Priorities
The Digital Mental Health Frontier
Opportunities
Challenges & Risks
Mental health apps reach millions: depression, anxiety, mindfulness, crisis support
AI and machine learning for early detection, personalized treatment, and monitoring
Digital phenotyping: passive data from smartphones to track mental state
Teletherapy and asynchronous text-based counseling increasing access
Chatbots (e.g., Woebot) showing promise for mild-moderate depression
Regulatory gap: most apps not evidence-based or clinically validated
Digital divide: unequal access by income, age, and geography
Data privacy and surveillance concerns
Risk of replacing human connection with technology
Algorithmic bias and under-performance for minority groups
Digital tools should complement — not replace — human-centered, rights-based care.
Section 8 · Future Directions
EMERGING PRIORITY
Climate Change & Mental Health
Direct Impacts
Heat-related psychological stress and aggression
Natural disaster trauma, PTSD, and displacement
Wildfires and flooding linked to acute stress disorders
"Eco-anxiety" — chronic worry about climate futures
Indirect Impacts
Loss of livelihoods and food insecurity → depression
Climate migration and community breakdown
Disruption of health services in disaster zones
Increased substance abuse in affected communities
Vulnerable Populations
Farmers, pastoralists, and fishing communities
Island nations and coastal populations
Indigenous communities with land-based identities
Children and young people facing climate futures
Mental Health Must Be Central to Climate Adaptation Plans
Include mental health in climate finance and national adaptation frameworks
Build psychological first aid capacity for disaster response
Address eco-anxiety in youth through education and meaningful action
Section 8 · Future Directions
Research Priorities for the Next Decade
Implementation Science
How do evidence-based interventions scale with fidelity in real-world settings?
LMIC-Led Research Agenda
Build capacity for locally-led, locally-relevant mental health research in the Global South
Social Determinants
Causal research linking poverty, inequality, and structural racism to mental health outcomes
Digital Health Evaluation
Rigorous RCTs and real-world studies of mental health apps and digital platforms
Neuroscience Meets Culture
Integrating biological and cultural/social determinants in mental health models
Long-Term Outcomes
Longitudinal studies tracking recovery, functioning, and quality of life — not just symptoms
Prevention Science
What prevents mental disorders? School, community, and policy-level interventions
Equity & Disparities
Research on intersectionality — race, gender, class, disability, and sexual orientation
Funding: Global mental health research receives <1% of total health research funding — a critical gap.
Section 8 · Future Directions
Ways Forward: A Call to Action
Invest adequately in mental health
— in budgets, workforce, and research, especially in LMICs
Decolonize the field
— center Global South voices, lived experience, and diverse knowledge systems
Scale what works
— task-sharing, community-based care, and evidence-based digital tools
Address root causes
— poverty, discrimination, adverse childhood experiences, and climate change
Uphold human rights
— eliminate coercion, promote autonomy, and enforce accountability
Build resilient systems
— integrated, adaptable, and recovery-oriented for the 21st century
“Mental health is not a luxury — it is a foundation for human dignity, development, and global equity.”
Thank you | Questions & Discussion
Global Mental Health: Discontents & Ways Forward
- global-mental-health
- public-health
- mental-health-policy
- who
- decolonization
- task-sharing
- digital-health