





Atopic Dermatitis: Clinical Overview and Management Guide
A comprehensive guide to eczema for medical professionals covering pathophysiology, age-based presentation, triggers, and pharmacological treatment ladders.
Atopic Dermatitis (Eczema): Clinical Overview
Pathophysiology, Diagnosis, and Management Protocols
For Medical Students & Clinicians
Prevalence: A Global Burden
Atopic Dermatitis is the most common chronic inflammatory skin disease, predominantly affecting the pediatric population.
60% of cases develop within the first year of life.
Associated with the 'Atopic March': Eczema → Food Allergy → Asthma → Rhinitis.
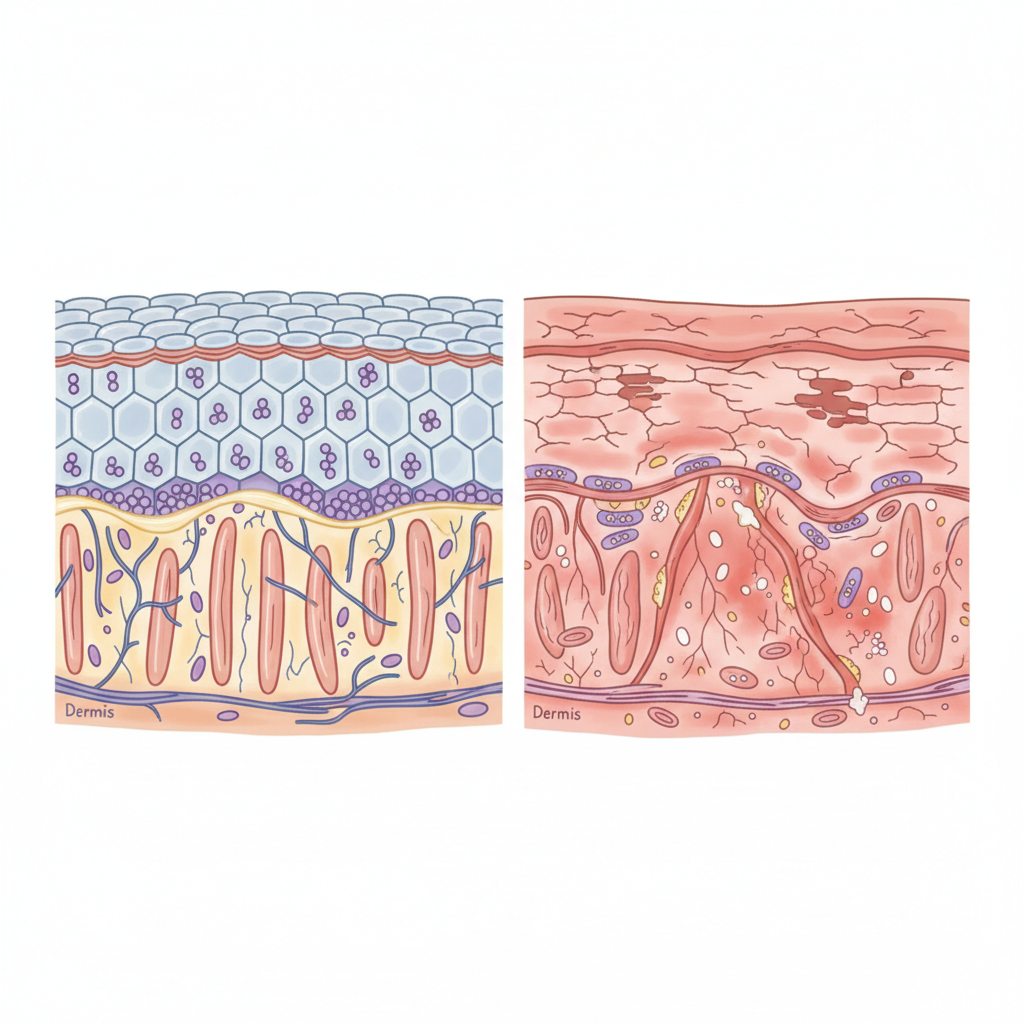
Pathophysiology: The Barrier Defect
Filaggrin Mutation: Loss of structural protein leading to defective stratum corneum.
Transepidermal Water Loss (TEWL): Increased moisture evaporation causes xerosis.
Immune Dysregulation: Th2 pathway dominance (IL-4, IL-13) drives inflammation.
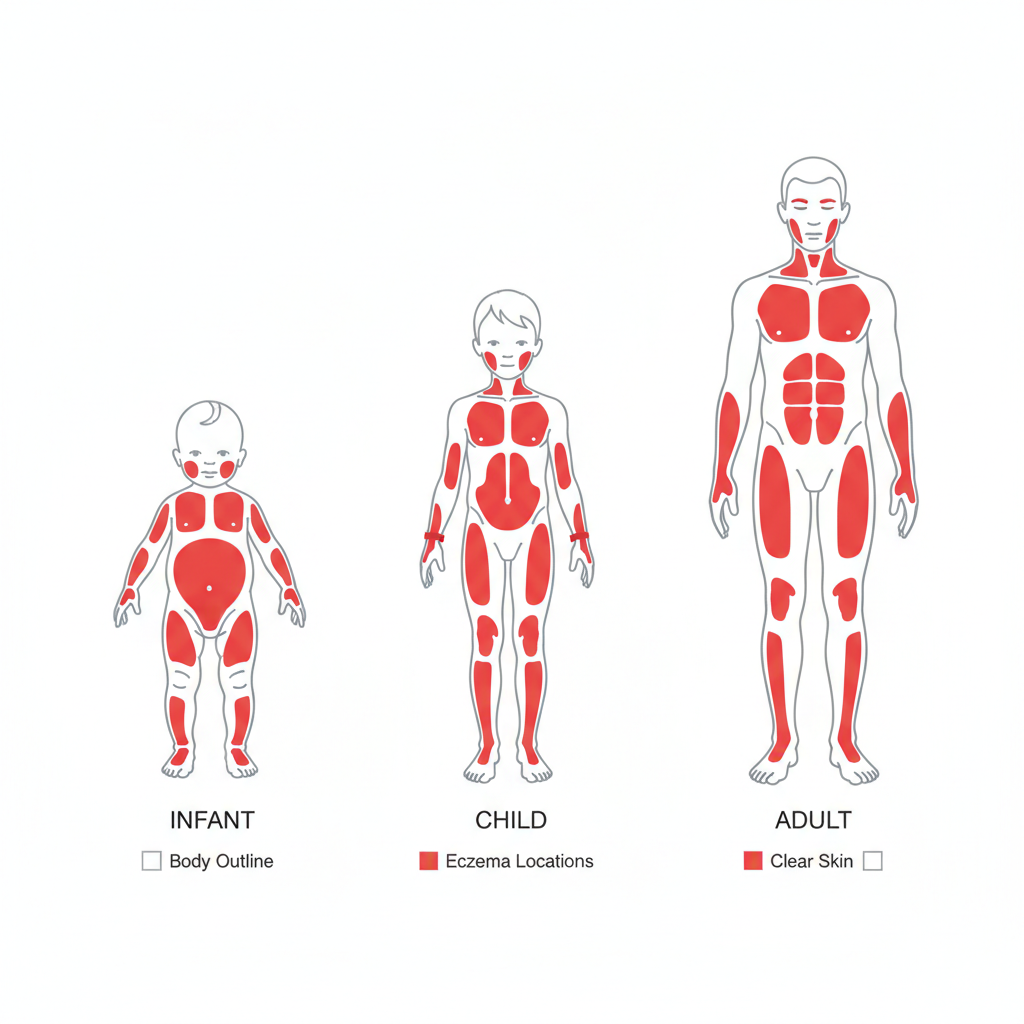
Clinical Presentation by Age
Infants
Extensor surfaces, face (cheeks), and scalp. Diaper area usually spared.
Children
Flexural folds (antecubital/popliteal fossae), neck, wrists.
Adults
Flexural areas, hands, face (eyelids), and nipples. Lichenification is common.
Common Triggers & Exacerbating Factors
Aeroallergens: Dust mites, pet dander, pollens.
Irritants: Wool, synthetic fabrics, harsh soaps, detergents.
Psychological: Stress and anxiety (triggers neuro-immune flare).
Environment: Extreme heat, humidity shifts, or dry cold air.
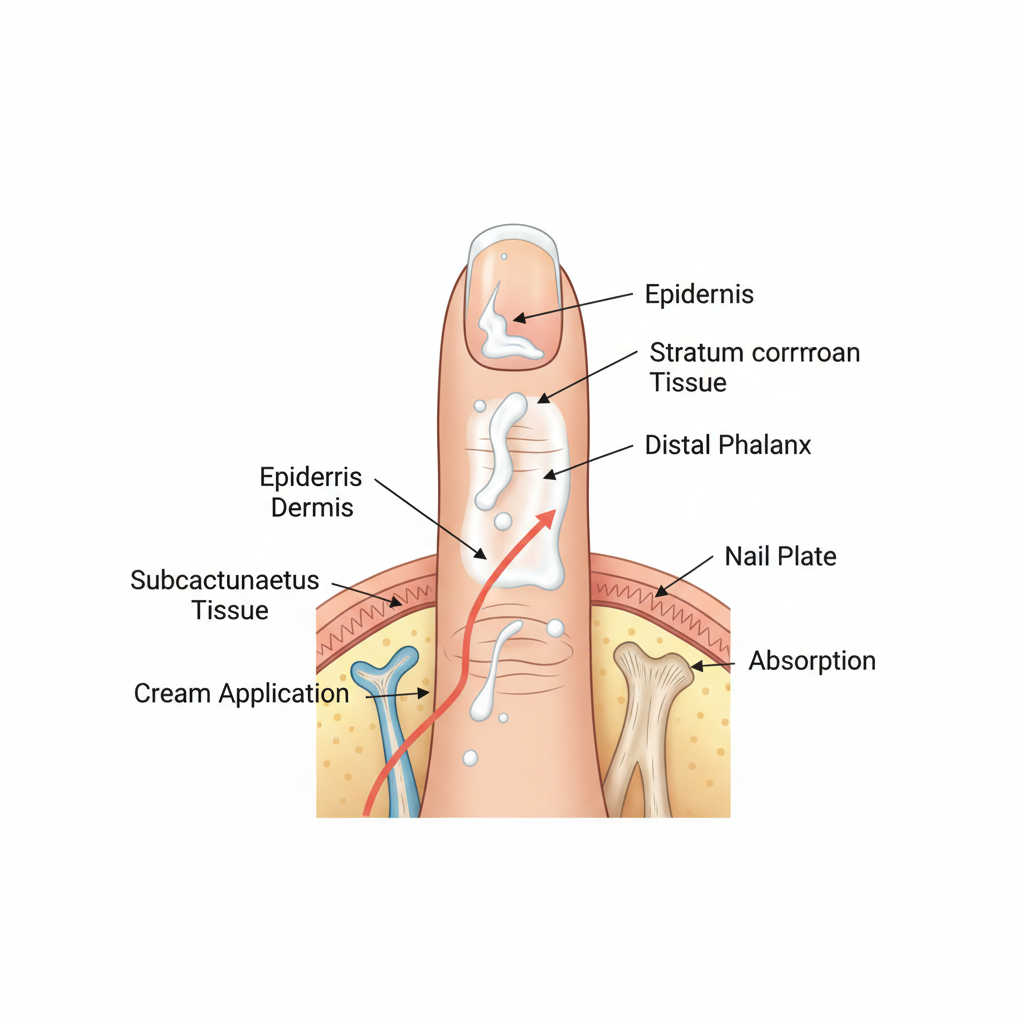
Daily Management: The Foundation
Aggressive Emollients
Apply thick creams/ointments (not lotions) at least twice daily. 'Soak and seal' method immediately after bathing.
Bathing Routine
Short (5-10 min), warm (not hot) baths. Use soap-free cleansers. Avoid scrubbing.
Pharmacological Management Ladder
Mild Disease
Low-potency TCS (e.g., Hydrocortisone 1-2.5%) for face/folds. Reactive therapy.
Moderate Disease
Medium-potency TCS (e.g., Triamcinolone). TCIs (Tacrolimus) for steroid-sparing. Proactive (weekend) therapy.
Severe/Refractory
High-potency TCS (short term). Phototherapy. Systemics: Dupilumab (Biologic), JAK Inhibitors, Cyclosporine.
Topical Corticosteroid Potency (USA Classification)
Class I (Super Potent)
Clobetasol propionate 0.05%
Class II-III (High Potency)
Betamethasone dipropionate 0.05%, Fluocinonide
Class IV-V (Mid Potency)
Triamcinolone acetonide 0.1%
Class VI-VII (Low Potency)
Desonide 0.05%, Hydrocortisone 1-2.5%
Dosing Rule: 1 Fingertip Unit (FTU) = ~0.5g = treats area of 2 adult palms.
Red Flags & Complications
1. Infection (S. aureus)
Weeping, honey-colored crusts (Impetiginization), pustules. Requires topical mupirocin or systemic antibiotics.
2. Eczema Herpeticum
EMERGENCY. Disseminated HSV infection. Monomorphic punched-out erosions, vesicles. Requires immediate Acyclovir.
Clinical Takeaways
Education is Key: Demonstrate 'Squeaky' vs 'Greasy' moisturizer application to parents.
Steroid Phobia: Address barely; undertreatment leads to chronic lichenification.
Maintenance: Proactive intermittent biologic/TCS use prevents relapse effectively.
- atopic-dermatitis
- eczema
- dermatology
- medical-education
- skin-disease
- clinical-protocols
- pediatrics