


Diabetic Foot Pathway: From Callus to Amputation
A clinical guide for healthcare professionals on diabetic foot management, covering neuropathy, ulcer classification, osteomyelitis, and MDT care.
The Diabetic Foot Pathway:<br>Callus to Amputation
Understanding the Progression, Prevention & Multidisciplinary Management
For Healthcare Professionals — Nurses, Podiatrists & GPs
Understanding the Diabetic Foot
15%
of patients with diabetes will develop a foot ulcer during their lifetime.
85%
of major lower extremity amputations are preceded by a non-healing foot ulcer.
#1
leading cause of non-traumatic lower-extremity amputations globally.
The Core Triad of Risk
Neuropathy
Ischemia
Infection
Foot<br>Ulcer
The interplay of loss of protective sensation, arterial insufficiency, and susceptibility to infection.
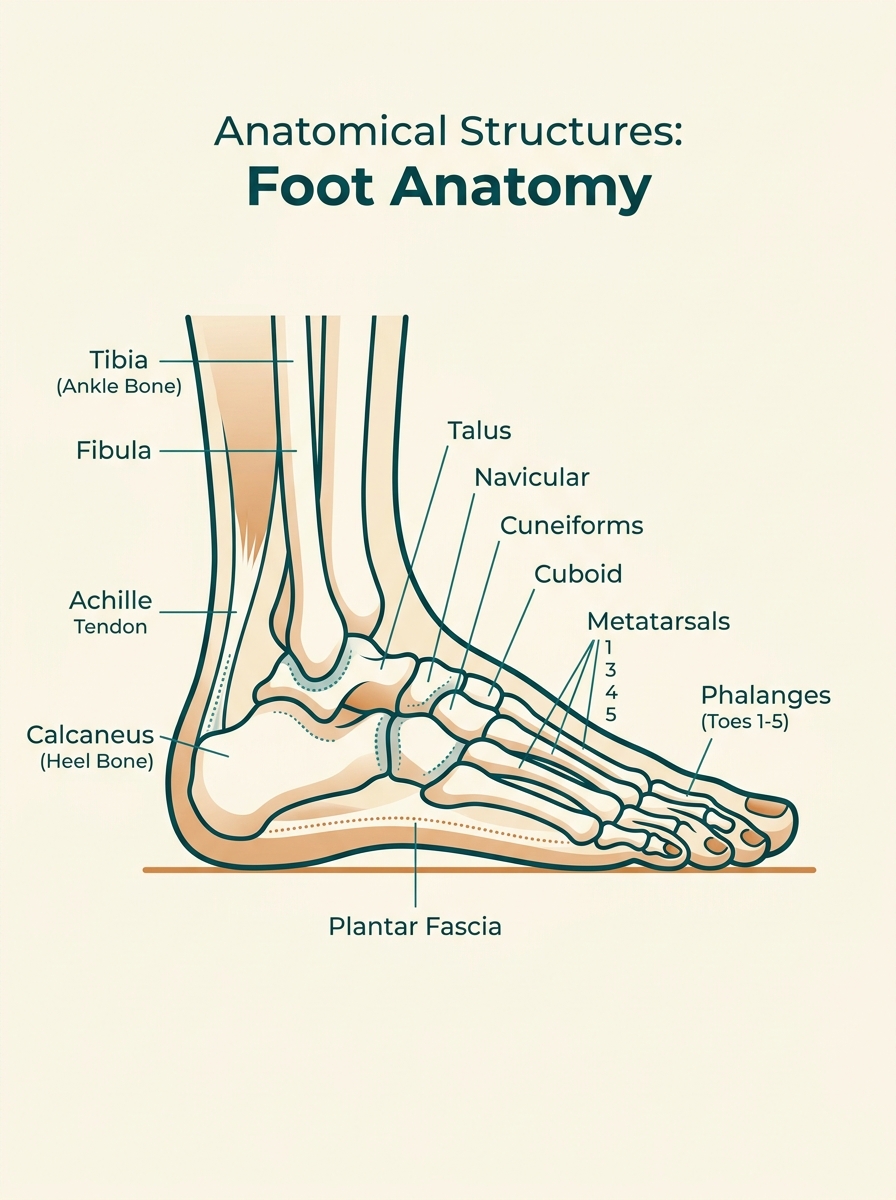
The Pathophysiology: Why Feet Fail in Diabetes
Peripheral Neuropathy
Loss of protective sensation (LOPS) masking injury
Motor neuropathy causing structural foot deformity
Autonomic neuropathy causing dry skin & fissures
Peripheral Arterial Disease
Significantly reduced blood flow to extremities
Impaired supply of vital oxygen and nutrients
Poor wound healing & increased risk of ischemia
Immunopathy
Impaired neutrophil and phagocytic cell function
Poor local inflammatory and infection response
Exacerbated risk under uncontrolled hyperglycemia
Callus: The Starting Point
What is callus?
Thickened skin resulting from repetitive pressure and friction.
Key Locations
Metatarsal heads, the heel, and the toes.
Why it matters in diabetes
Masks underlying ulceration
Increases plantar pressure by up to 30%
Acts as a pre-ulcerative lesion
Clinical Assessment
Inspect feet regularly and ensure prompt professional debridement.
Prevention
Implement optimal offloading and targeted appropriate footwear.
Diabetic Foot Ulcers: Classification & Assessment
Wagner Grade System (0-5)
Pre/post<br>ulcer
Superficial<br>ulcer
Deep to tendon<br>or capsule
Deep with<br>osteomyelitis
Partial<br>gangrene
Full foot<br>gangrene
Key Assessment Pillars
Also see: SINBAD & University of Texas Systems
Wound Size
Ulcer Depth
Infection Signs
Vascularity
Sensation
Infection in the Diabetic Foot
Breakdown of the skin barrier (typically via chronic ulceration)
Frequently polymicrobial (involving multiple bacterial strains)
Clinical Tip: Patients may lack classic signs (e.g., pain) due to peripheral neuropathy.
Look for: localized redness, warmth, swelling, or purulent discharge (pus).
A positive probe-to-bone test strongly suggests underlying osteomyelitis.
Fever • Systemic Sepsis • Crepitus • Rapidly Spreading Cellulitis
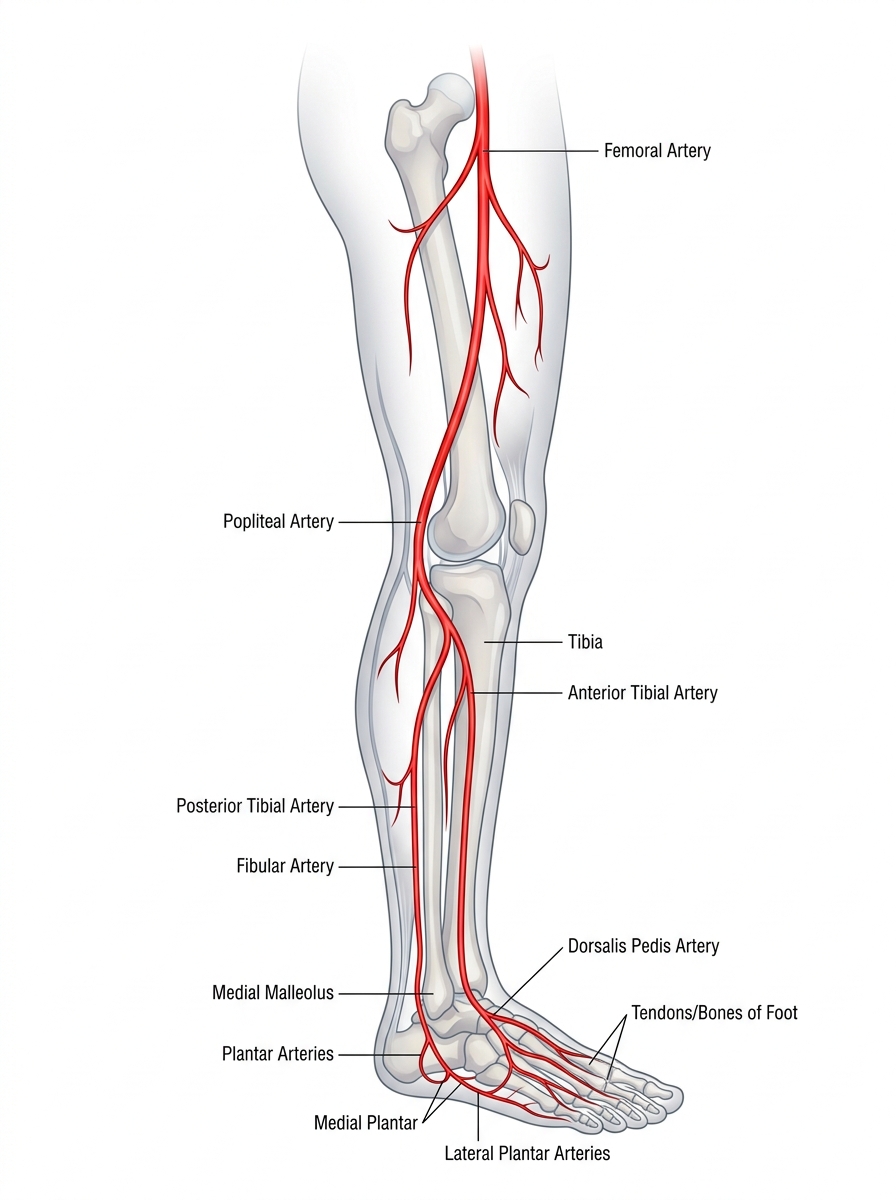
Vascular Assessment & Ischemia
Timely vascular assessment is crucial in evaluating Diabetic Foot Ulcers (DFU) to determine healing potential and prevent lower extremity amputation.
Osteomyelitis: Bone Deep
Definition & Mechanism
<b>Bone infection</b> — a limb-threatening complication.<br>It occurs predominantly via <b>contiguous spread</b> from soft tissue in Diabetic Foot Ulcers.
Diagnosis
<ul style='margin: 0; padding-left: 20px;'><li style='margin-bottom: 15px;'><b>Probe-to-bone test</b> <span style='font-size: 22px; color: #D16D54;'>(sensitivity 89%)</span></li><li style='margin-bottom: 15px;'><b>Plain X-ray</b> <span style='font-size: 22px; color: #888888;'>(late changes)</span></li><li style='margin-bottom: 15px;'><b>MRI</b> <span style='font-size: 22px; color: #D16D54;'>(gold standard)</span></li><li style='margin-bottom: 0;'><b>Bone biopsy</b></li></ul>
Treatment Strategy
<ul style='margin: 0; padding-left: 20px;'><li style='margin-bottom: 15px;'><b>Prolonged antibiotics</b> <span style='font-size: 22px; color: #D16D54;'>(6 weeks+)</span></li><li style='margin-bottom: 15px;'><b>Surgical debridement</b></li><li style='margin-bottom: 0;'><b>Possible ray amputation</b></li></ul>
Early diagnosis is critical to avoid major amputation.
The Multidisciplinary<br>Team Approach
A collaborative, patient-centered model for managing diabetic foot disease covering prevention to surgical intervention.
Core MDT Members
Podiatrist
Debridement, offloading & wound care
Diabetologist
Glycaemic control & systemic management
Vascular Surgeon
Revascularization & tissue perfusion
Orthopaedic Surgeon
Bone/joint intervention & amputation
Infectious Disease
Microbiology & antibiotic stewardship
Wound Care Nurse
Specialist dressings & daily monitoring
Orthotist
Custom footwear & offloading devices
General Practitioner
Care coordination & primary prevention
Amputation: When & Why
Minor Amputation
Toe, ray, transmetatarsal
Major Amputation
Below-knee, above-knee
Pre & Post-Amputation Care
Uncontrollable infection
Critical ischemia
Non-healing wound
Patient choice
Aim for most distal level possible
Vascular assessment before surgery
Stump healing considerations
Psychological Support
Physiotherapy
Prosthetics
Rehabilitation
Prevention: Breaking the Cycle
Regular Screening
Annual foot screening for all diabetic patients, and 3-monthly reviews for those at high risk.
Patient Education
Teaching essential foot care, appropriate footwear choices, and the rule to never walk barefoot.
Glycaemic Control
Maintaining strict HbA1c targets to minimise neuropathy and peripheral vascular complications.
Pressure Offloading
Using total contact casting and therapeutic footwear to safely relieve pressure areas.
Early Referral
Establishing rapid pathways ensuring any new ulcer is seen by specialist podiatry within 24 hours.
Risk Stratification
Categorising patients actively into NICE/IWGDF low, moderate, high, or active disease statuses.
Early detection and prompt action saves limbs and lives.
Key Takeaways
<strong style="color: #222222;">Callus is not benign</strong> — it signals high pressure and risk of ulceration
<strong style="color: #222222;">Neuropathy, ischemia and infection</strong> are the triad driving diabetic foot disease
<strong style="color: #222222;">Classify every ulcer</strong> — Wagner or SINBAD grading guides management
<strong style="color: #222222;">Infection can be silent</strong> in diabetics — always probe, assess, and image
<strong style="color: #222222;">MDT coordination is essential</strong> at every stage of the pathway
<strong style="color: #222222;">Prevention and early referral</strong> are the most powerful tools we have
References: <span style="color: #555555; font-weight: 400;">NICE NG19 • IWGDF Guidelines 2023 • Diabetes UK</span>
- diabetes
- foot-care
- wound-management
- podiatry
- nursing
- diabetic-ulcer
- healthcare-education