





Biopsychosocial Approach to Pain in Physiotherapy
Explore pain physiology, psychological coping strategies, and effective communication models like OARS and Regulatory Focus for modern physiotherapy.
Pain Physiology & Psychology: A Biopsychosocial Approach
Patient Communication, Coping Strategies, and Regulatory Focus in Physiotherapy
Pain Physiology: The 4 Stages
<ul><li><strong>Transduction:</strong> Nociceptors convert tissue damage (thermal, mechanical, chemical) into electrical signals.</li><li><strong>Transmission:</strong> Signals travel via A-delta (fast) and C-fibers (slow) to the spinal cord and brain.</li><li><strong>Modulation:</strong> Descending pathways can inhibit or facilitate the pain signal (Gate Control Theory).</li><li><strong>Perception:</strong> The brain integrates sensory input to create the subjective experience of pain.</li></ul>
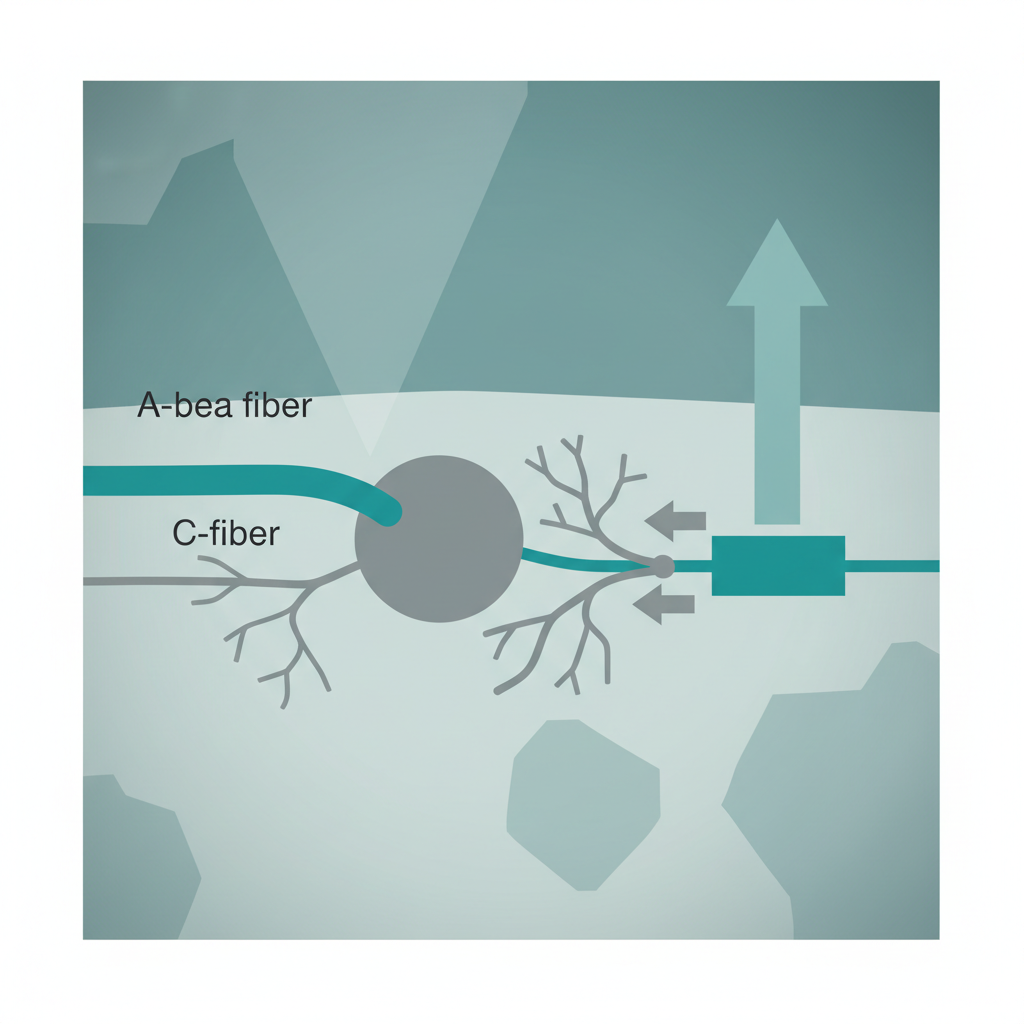
The Gate Control Theory
<ul><li><strong>Mechanism:</strong> Proposed by Melzack & Wall (1965). Pain modulation occurs in the dorsal horn of the spinal cord (Substantia Gelatinosa).</li><li><strong>Closing the Gate:</strong> Non-painful input (A-beta fibers, e.g., rubbing, vibration) activates inhibitory interneurons, blocking pain signals.</li><li><strong>Opening the Gate:</strong> Intense pain signals (C-fibers) or descending facilitation (anxiety, fear) inhibit the interneurons, allowing pain ascent.</li><li><strong>Clinical Relevance:</strong> Explains why massage, TENS, and movement can effectively reduce pain perception.</li></ul>
Nociception ≠ Pain
Nociception is the 'danger signal' sent to the system, but pain is the output generated by the brain. A dangerous situation (e.g., snake bite) might yield no pain due to adrenaline, while a minor input (twig scratch) can cause severe pain if perceived as a threat.
Chronic Pain: Central Sensitization
In chronic pain, the central nervous system becomes hypersensitive. This leads to Hyperalgesia (increased pain from painful stimuli) and Allodynia (pain from non-painful stimuli). The brain's 'alarm system' is stuck in the 'on' position.
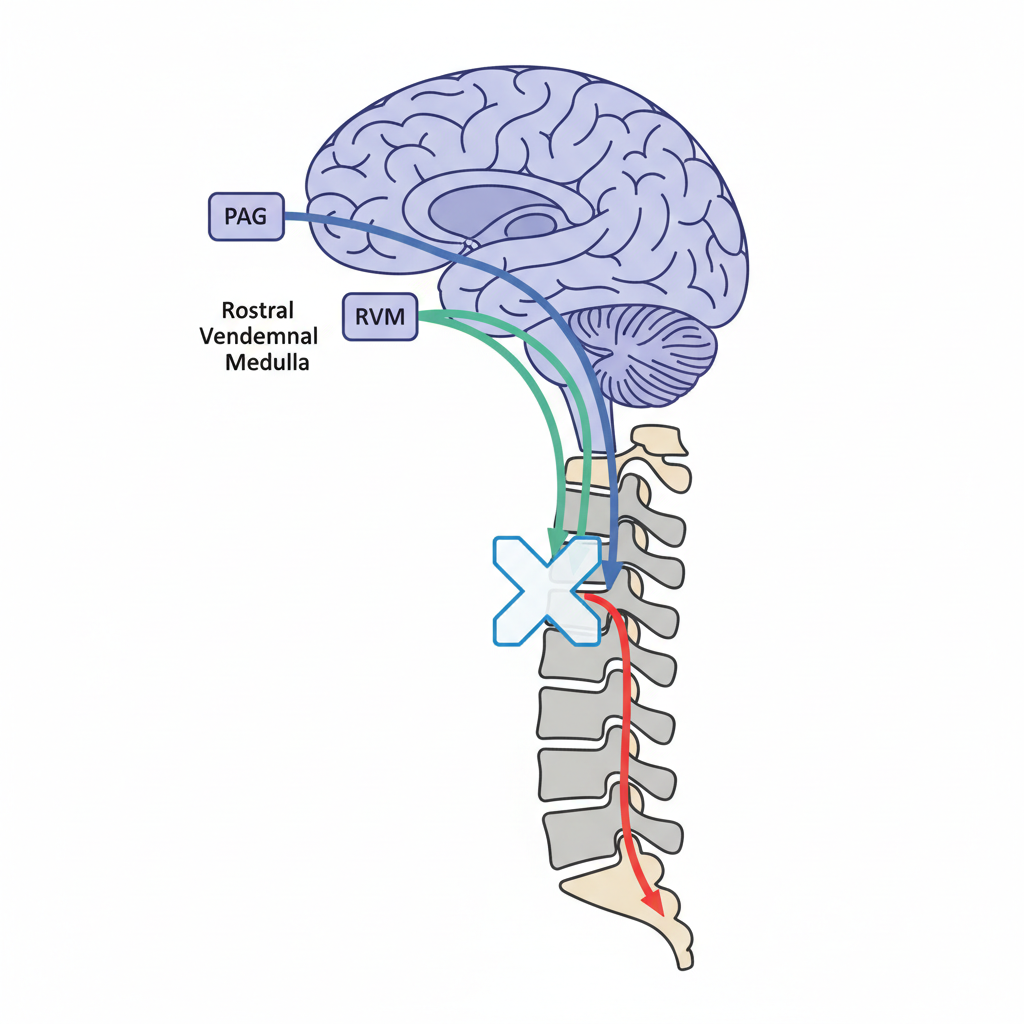
Descending Pain Modulation
<ul><li><strong>The Brain's Control Mechanism:</strong> The brain isn't just a receiver; it controls the volume of pain.</li><li><strong>Key Structures:</strong> Periaqueductal Gray (PAG) and Rostral Ventromedial Medulla (RVM).</li><li><strong>Neurotransmitters:</strong> Serotonin, Norepinephrine, and Endogenous Opioids.</li><li><strong>Implication:</strong> Thoughts, emotions, and expectations can trigger these pathways to inhibit (block) or facilitate (amplify) pain.</li></ul>
The Brain as an Orchestra
The brain is like a skilled orchestra capable of playing thousands of melodies.
Pain is just one melody. In chronic pain, the orchestra plays the same melody repeatedly.
The musicians (neurons) lose their creativity and ability to play new songs (joy, curiosity).
The Biopsychosocial Model of Pain
Focuses on tissue damage, generic factors, neurophysiology, and inflammatory processes. Traditionally the sole focus of medicine, but insufficient for chronic pain.
Includes thoughts, beliefs (catastrophizing), emotions (fear, depression), coping strategies, and memory of past experiences. Strongly influences pain intensity.
Contextual factors: work environment, family support, socioeconomic status, and cultural beliefs about pain. These dictate the external stressors and resources.
The Fear-Avoidance Model
Psychological factors like catastrophizing and vigilance amplify pain perception. Fear leads to avoidance, which causes physical deconditioning and mood changes (depression, anxiety), further fueling the pain.
Effective Communication Strategies
<h3>Validation & Empathy</h3><p>Validate the patient's experience. Pain is real, regardless of tissue damage status. Use empathetic listening to lower the 'threat' level.</p>
<h3>Education (Neuroscience)</h3><p>Explain 'Hurt ≠ Harm'. Teach patients about neuroplasticity to instill hope. reducing fear lowers central sensitization.</p>
<h3>Reframing Beliefs</h3><p>Shift from a 'biomedical' fix-it view to a 'biopsychosocial' management view. Encourage focus on function over pain scores.</p>
Psychological Defense Mechanisms
Defense mechanisms are unconscious protections against anxiety. Physios must recognize these to guide patients toward conscious coping.
<ul><li><strong>Regression:</strong> Returning to a childlike state of dependency.</li><li><strong>Projection:</strong> Attributing one's own frustration/anger to the therapist or others.</li><li><strong>Denial:</strong> Refusing to acknowledge the reality of a chronic condition.</li><li><strong>Rationalization:</strong> Creating logical excuses for avoidance behavior.</li></ul>
Pain Catastrophizing
<p>A negative mental set affecting pain outcome, characterized by:</p><ul><li><strong>Rumination:</strong> "I can't stop thinking about how much it hurts."</li><li><strong>Magnification:</strong> "I'm afraid that something serious is wrong."</li><li><strong>Helplessness:</strong> "There is nothing I can do to reduce the pain."</li></ul><p><strong>Impact:</strong> Higher pain intensity, increased disability, and poorer response to treatment.</p>
Lazarus Transactional Model of Stress
<strong>Primary Appraisal</strong><br>Is this stressor a threat? (e.g., "Is this pain dangerous?")
<strong>Secondary Appraisal</strong><br>Do I have the resources to cope? (e.g., "Can I manage this?")
<strong>Coping Response</strong><br>Problem-focused (change situation) or Emotion-focused (change regulation).
Sense of Coherence (Antonovsky)
Antonovsky proposes that health is maintained through a 'Sense of Coherence' (SOC). For pain management, patients need:
Coping Strategies: Adaptive vs. Maladaptive
<strong>Adaptive:</strong> Task-persistence, deflection, seeking social support, relaxation.<br><strong>Maladaptive:</strong> Guarding, resting, catastrophizing, isolation.
Active vs. Passive Coping
<h3 style='color:#2a9d8f; text-align:center;'>Active Strategies</h3><ul style='font-size:24px; line-height:1.6;'><li>Physical Activity / Exercise</li><li>Relaxation techniques</li><li>Task persistence (pacing)</li><li>Seeking social support</li><li><strong>Outcome:</strong> Lower disability, higher self-efficacy.</li></ul>
<h3 style='color:#e76f51; text-align:center;'>Passive Strategies</h3><ul style='font-size:24px; line-height:1.6;'><li>Relying on medication</li><li>Resting / Avoiding activity</li><li>Relying on doctors for a "cure"</li><li>Wishful thinking</li><li><strong>Outcome:</strong> Higher disability, depression.</li></ul>
<p><strong>Clinical Goal:</strong> Shift patients from passive recipients of care to active participants.</p><p>This reduces catasrophizing and helplessness, fostering long-term resilience and independence.</p>
Motivational Interviewing: The OARS Model
Regulatory Focus Theory in Pain
<h3 style='color:#2a9d8f'>Promotion Focus</h3><ul><li>Focus on <strong>Gains</strong> and Aspirations.</li><li>Goal: Repaid recovery, getting back to sport/work.</li><li>Strategy: Eager approach.</li><li><em>Physio Tip:</em> Set goals related to 'what you will be able to do'.</li></ul>
<h3 style='color:#e76f51'>Prevention Focus</h3><ul><li>Focus on <strong>Non-Losses</strong> and Security.</li><li>Goal: Avoiding further injury, safety.</li><li>Strategy: Vigilant avoidance.</li><li><em>Risk:</em> Higher anxiety and hypervigilance in chronic pain.</li></ul>
Tailoring Messages: Regulatory Fit
<h3 style='color:#2a9d8f; text-align:center;'>For Promotion-Focused Patients</h3><p style='font-size:24px; color:#555;'><strong>Emphasize Achievement & Growth:</strong></p><ul style='font-size:22px; line-height:1.5;'><li>"This exercise will help you <strong>run faster</strong>."</li><li>"Doing this gets you back to <strong>work sooner</strong>."</li><li>"Imagine the <strong>progress</strong> you can make."</li></ul>
<h3 style='color:#e76f51; text-align:center;'>For Prevention-Focused Patients</h3><p style='font-size:24px; color:#555;'><strong>Emphasize Safety & Protection:</strong></p><ul style='font-size:22px; line-height:1.5;'><li>"This exercise will <strong>prevent</strong> stiffness."</li><li>"Doing this helps you <strong>avoid</strong> flare-ups."</li><li>"This ensures your back stays <strong>safe</strong>."</li></ul>
Practical Application in Rehabilitation
<ul><li><strong>Early Screening:</strong> Assess for yellow flags (fear avoidance, catastrophizing) in the first session.</li><li><strong>Tailored Education:</strong> Use metaphors relevant to the patient. Explain mechanisms, not just anatomy.</li><li><strong>Goal Setting:</strong> Align with the patient's Regulatory Focus. <br><em>Promotion:</em> "Let's get back to running."<br><em>Prevention:</em> "Let's stop the pain from getting worse."</li><li><strong>Graded Exposure:</strong> Step-by-step reintroduction to feared movements.</li></ul>
Conclusion: A Comprehensive Approach
<ul><li>Pain is a multisystem output of the brain, not just a measure of tissue damage.</li><li>Psychological factors (fear, avoidance, catastrophizing) modulate the pain experience.</li><li>Effective physiotherapy requires moving beyond the biomedical model to a biopsychosocial one.</li><li>Communication is a therapeutic intervention: Validate, Educate, and Reframe.</li><li>Understanding coping styles and regulatory focus allows for tailored patient care.</li></ul>
- physiotherapy
- pain-management
- biopsychosocial-model
- chronic-pain
- patient-communication
- psychology
- rehabilitation