Anti-Fungal Agents in Dermatology: Pharmacology & Use
Explore the mechanisms, classification, and clinical applications of antifungal drugs like Azoles and Terbinafine in dermatological practice.
Anti-Fungal Agents in Dermatology
Pharmacology, Mechanisms, and Clinical Applications for MBBS
Based on standard Pharmacology references (K.D. Tripathi, Katzung)
Introduction to Mycoses
Fungal infections (mycoses) in dermatology are primarily superficial, affecting the skin, hair, and nails. Unlike bacteria, fungi are eukaryotes with rigid cell walls containing chitin and cell membranes containing ergosterol. This biochemical difference is the primary target for selective toxicity in anti-fungal pharmacotherapy.
Classification of Anti-Fungal Drugs
<b>Antibiotics:</b> Polyenes (Amphotericin B, Nystatin) and Heterocyclic Benzofuran (Griseofulvin).
<b>Antimetabolites:</b> Flucytosine (5-FC).
<b>Azoles:</b> Imidazoles (Ketoconazole, Clotrimazole) and Triazoles (Fluconazole, Itraconazole).
<b>Allylamines:</b> Terbinafine, Naftifine (Inhibit squalene epoxidase).
Polyenes: Mechanism of Action
Polyenes like Amphotericin B bind tightly to <b>ergosterol</b> present in the fungal cell membrane. They do not bind to mammalian cholesterol with the same affinity. This binding forms micropores in the membrane, leading to the leakage of intracellular ions (K+) and macromolecules, ultimately causing cell death (Fungicidal action).
Azoles: Mechanism of Action
Azoles are fungistatic agents that inhibit the fungal cytochrome P450 enzyme <b>lanosterol 14-alpha-demethylase</b>. This inhibition blocks the conversion of lanosterol to ergosterol. The depletion of ergosterol alters membrane fluidity and accumulates toxic 14-alpha-methyl sterols, inhibiting growth.
Systemic Azoles: Fluconazole vs. Itraconazole
<b>Fluconazole:</b> Water-soluble, >90% bioavailability, excellent CSF penetration. Drug of choice for Candida infections and Cryptococcal meningitis. Not effective against filamentous molds (Aspergillus).
<b>Itraconazole:</b> Lipid-soluble, requires acidic pH for absorption. Broader spectrum (includes Aspergillus and Dermatophytes). Accumulates in skin and nails (reservoir effect).
<b>Interactions:</b> Both inhibit CYP450 enzymes, leading to potential toxicity when combined with drugs like warfarin or statins.
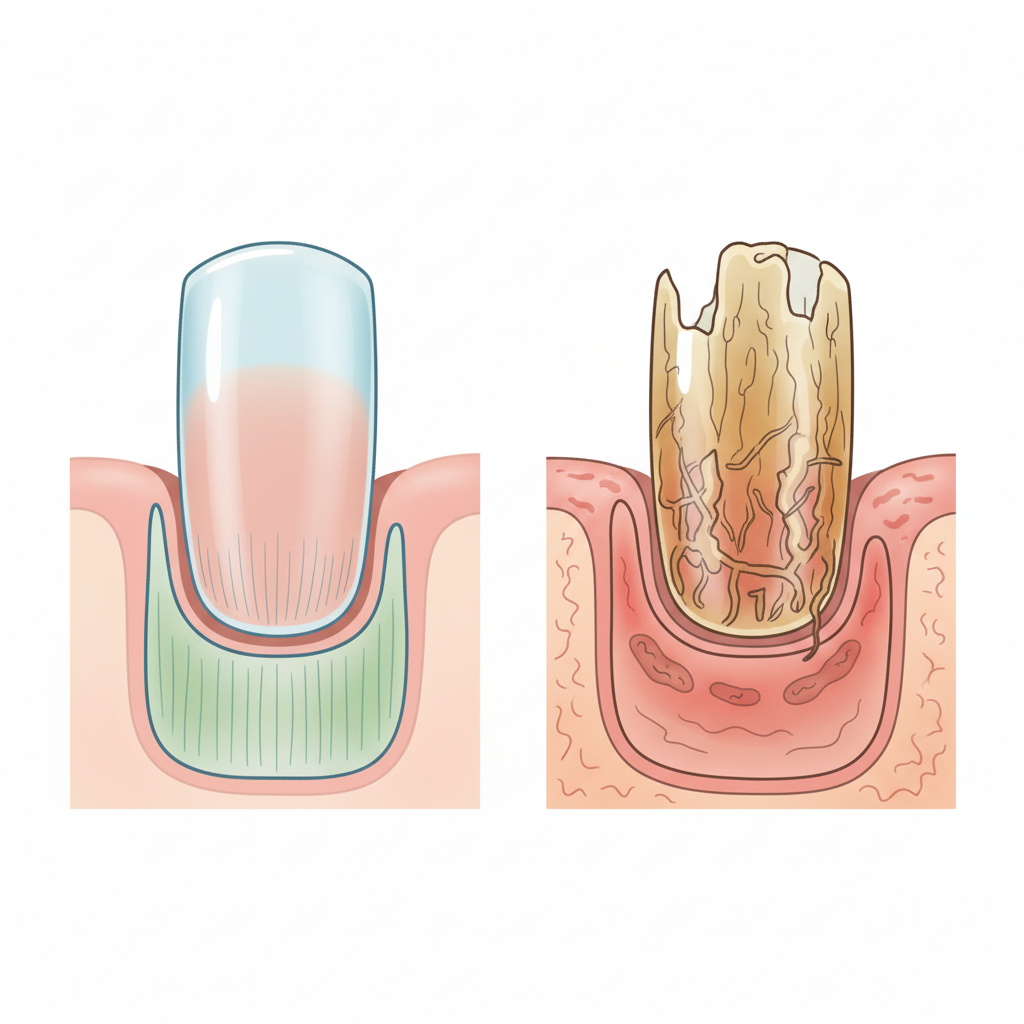
Allylamines: Terbinafine
<b>Mechanism:</b> Inhibits squalene epoxidase, an early step in ergosterol biosynthesis. This leads to the accumulation of squalene, which is toxic to the fungal cell.<br><br><b>Clinical Use:</b> It is fungicidal and highly lipophilic, accumulating in keratin. It is the gold standard for treating Onychomycosis (nail fungus) and dermatophytosis.
Griseofulvin is a 'keratophilic' drug. It binds to microtubular proteins in the nucleus, disrupting the mitotic spindle and inhibiting fungal mitosis.
Historical Note: First isolated from Penicillium griseofulvum. Use has declined due to newer agents but remains relevant for Tinea Capitis in children.
Oral Bioavailability Comparison
Bioavailability varies significantly among systemic antifungals. Fluconazole and Voriconazole have excellent absorption, whereas Itraconazole is variable (approx 55%) and dependent on gastric acidity.
Topical Anti-Fungal Agents
<b>Clotrimazole & Miconazole:</b> Broad-spectrum topical azoles used for Tinea corporis, Tinea cruris, and Tinea pedis. Generally applied twice daily.
<b>Nystatin:</b> A polyene too toxic for systemic use but excellent specifically for <i>Candida</i> infections of skin and mucous membranes.
<b>Ciclopirox Olamine:</b> A broad-spectrum agent with a unique mechanism (iron chelation). Used in nail lacquers for mild Onychomycosis and anti-dandruff shampoos.
Clinical Treatment Guidelines
<b>Tinea Capitis:</b> Requires systemic therapy. Griseofulvin (children) or Terbinafine.
<b>Onychomycosis:</b> Oral Terbinafine (6 weeks for fingernails, 12 weeks for toenails). Pulse therapy with Itraconazole is an alternative.
<b>Candidiasis:</b> Topical Azoles/Nystatin for cutaneous. Oral Fluconazole for vaginal or extensive mucocutaneous infections.
<b>Tinea Versicolor:</b> Selenium sulfide or Ketoconazole shampoo; oral Fluconazole in resistant cases.
Summary & Key Points
Antifungal therapy targets unique fungal structures (Ergosterol, Cell Wall). Polyenes (Amphotericin B) are fast-acting fungicidal agents but toxic. Azoles are safer, broad-spectrum choices for systemic use but require careful monitoring for CYP450 interactions. Terbinafine is the agent of choice for dermatophytes. Correct diagnosis determines the choice between topical and systemic therapy.
- pharmacology
- dermatology
- antifungals
- medical-education
- terbinafine
- azoles
- mycoses