





Pediatric Nursing: Eye and Ear Sensory Disorders
Comprehensive guide to pediatric nursing care for visual and auditory disorders, including Acute Otitis Media, strabismus, and cataracts.
Anatomic Differences in Pediatrics
<strong>The Eye:</strong> Visualization is not fully developed until age 7. Eyeball occupies larger space within orbit, making it more susceptible to injury.
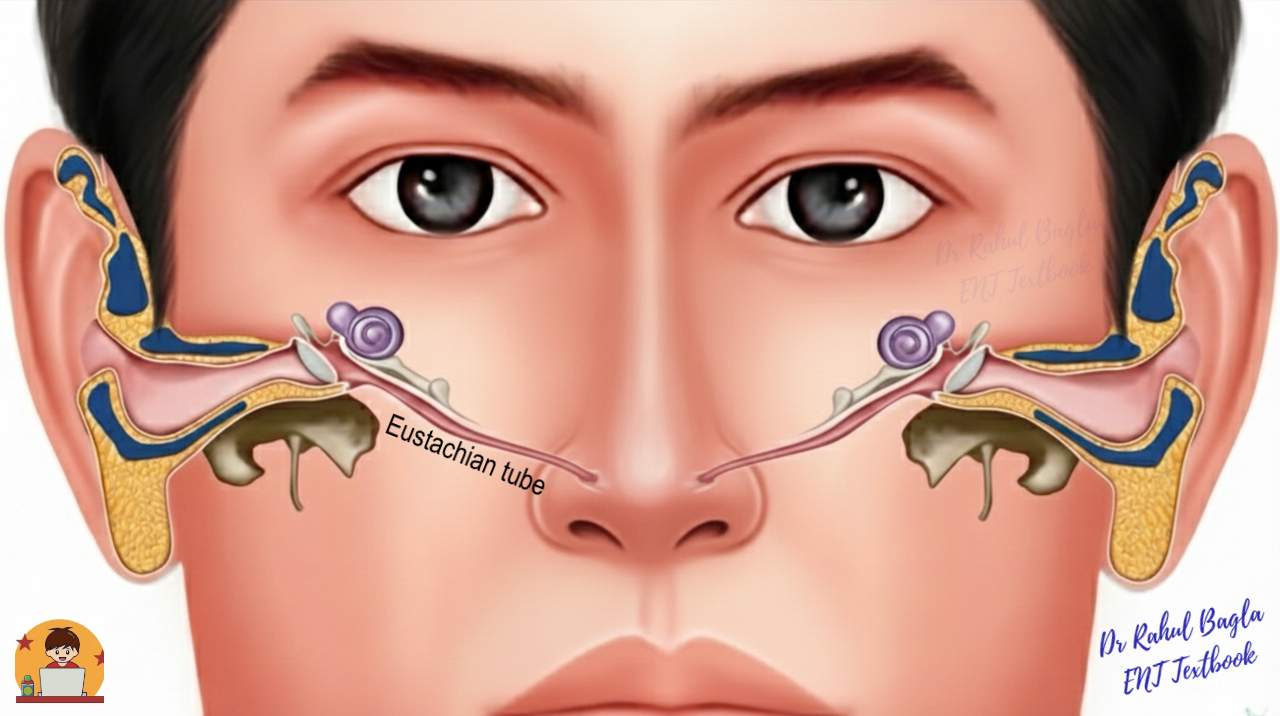
<strong>The Ear:</strong> Eustachian tubes are shorter, wider, and more horizontal in infants.
<strong>Implication:</strong> Horizontal inhibited drainage creates a risk factor for pathogen entry and otitis media.
Diagnostic Assessment Findings
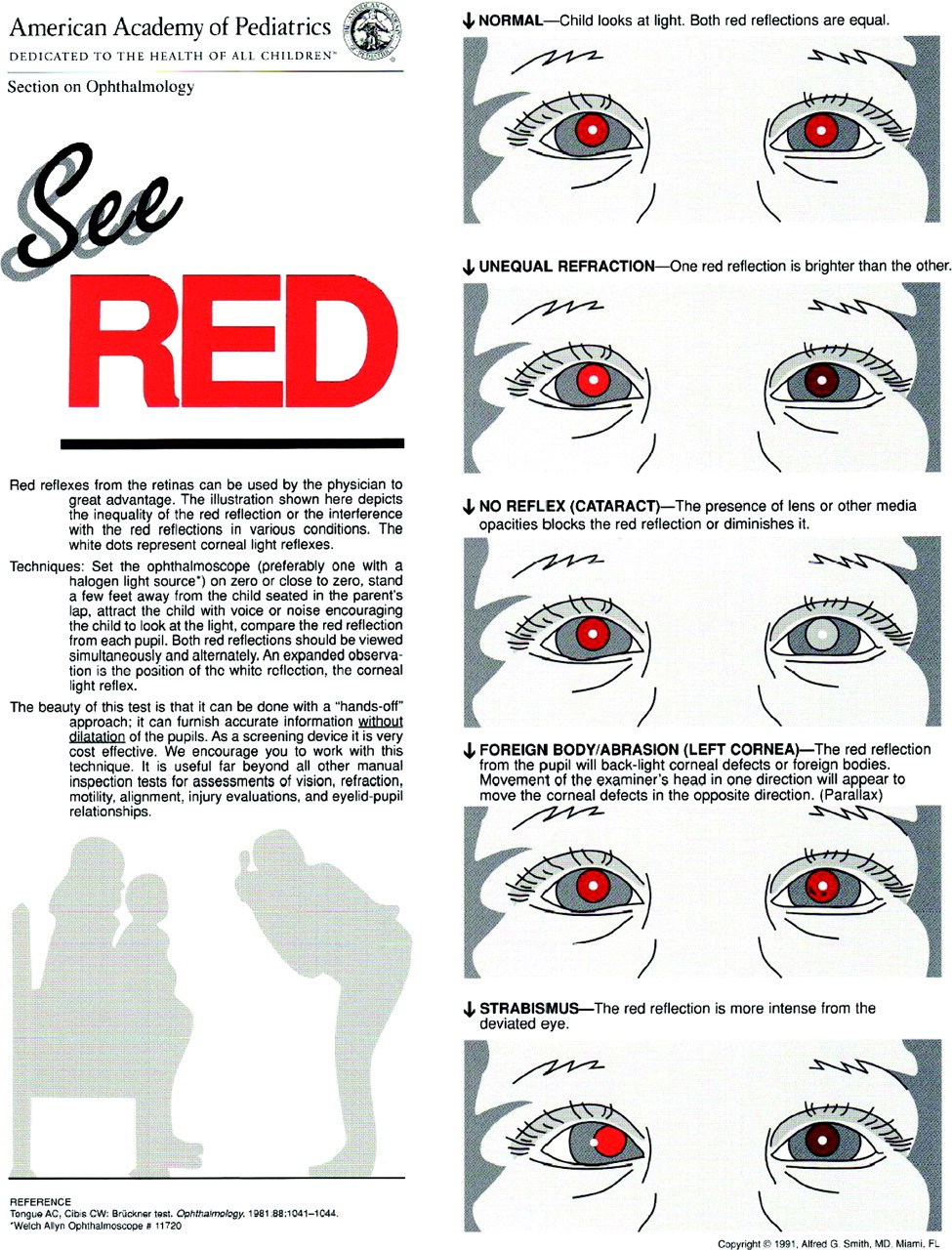
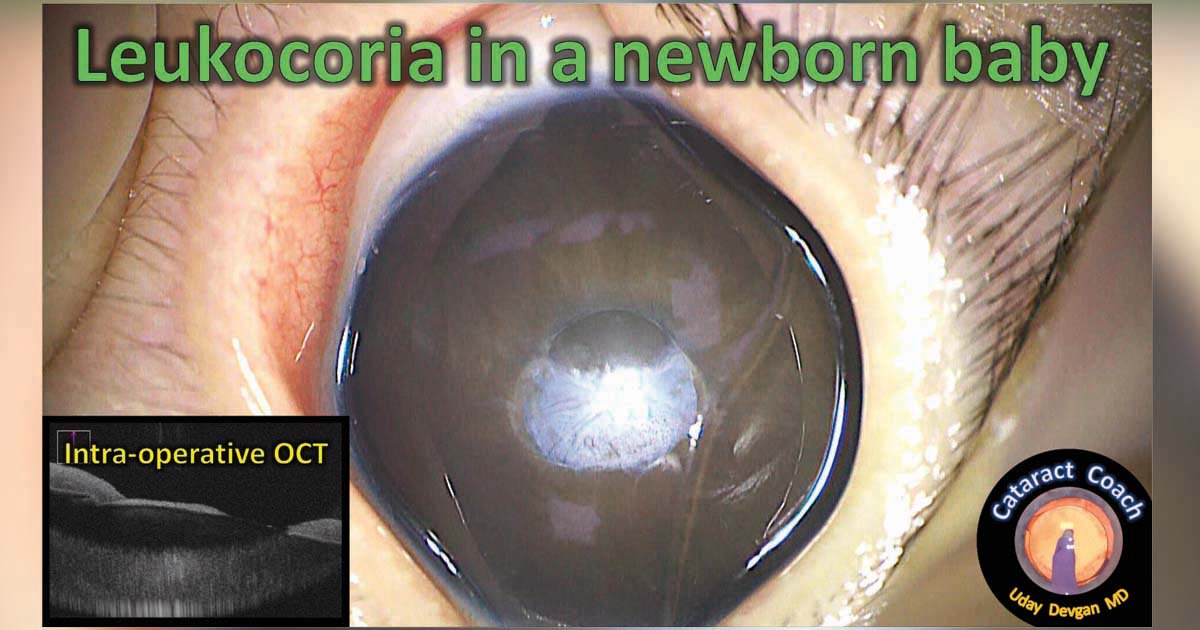
<ul><li><strong>Uncover-Cover Test:</strong> Assesses for strabismus and muscle fixation.</li><li><strong>Red Reflex:</strong> Crucial newborn screening; absence (leukocoria) may indicate cataracts or retinoblastoma.</li><li><strong>Pneumatic Otoscopy:</strong> Assesses tympanic membrane mobility and fluid presence.</li><li><strong>Tympanometry:</strong> Measures middle ear pressure to confirm effusion.</li></ul>
Common Infectious Eye Disorders
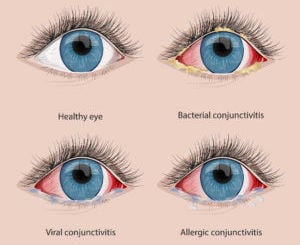
Conjunctivitis ('Pink Eye')
<ul><li><strong>Bacterial:</strong> Purulent discharge, eyelids stuck shut upon waking. Tx: Topical antibiotics.</li><li><strong>Viral:</strong> Watery discharge, lymphadenopathy, self-limiting.</li><li><strong>Allergic:</strong> Itching, watery, bilateral. Tx: Antihistamines.</li></ul>
Periorbital (Preseptal) Cellulitis
<ul><li>Infection of eyelid and surrounding tissue.</li><li><strong>S/S:</strong> Swollen, tender, red/purple eyelid; restricted eye movement is a red flag (orbital cellulitis).</li><li><strong>Mgmt:</strong> Systemic antibiotics (IV for severe cases), warm compresses.</li></ul>
Refractive Errors & Management
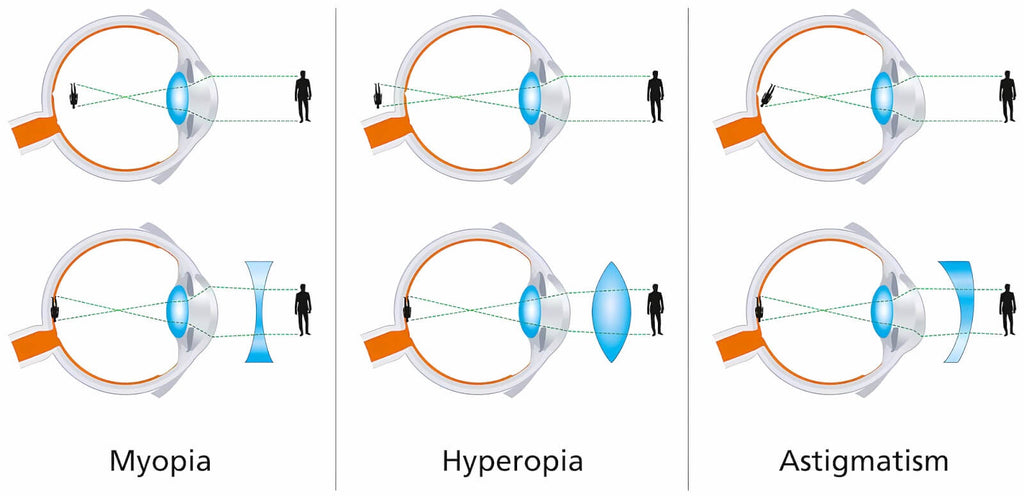
Hyperopia (Farsightedness)
Light focuses behind the retina. Normal in preschoolers, usually resolves.
Myopia (Nearsightedness)
Light focuses before the retina. Difficulty seeing distance (e.g., the board).
Astigmatism
Uneven curvature of cornea/lens causing blurred vision at all distances.
Motility Disorders: Strabismus & Amblyopia
<strong>Strabismus (Misalignment):</strong><br>Exotropia (outward) or Esotropia (inward). Brain suppresses image from weak eye to avoid double vision.
<strong>Amblyopia (Lazy Eye):</strong><br>Reduced visual acuity resulting from untreated strabismus. The brain permanently ignores the eye if not corrected by age 6-7.
<strong>Priority Intervention - Patching (Occlusion Therapy):</strong><br>Patch the GOOD eye to force the WEAK eye to work. Compliance is the #1 nursing challenge.
Critical Congenital & Acquired Disorders
<strong>Congenital Cataracts:</strong><br>Opacity of the lens. Must be removed surgically (often <2 months age) to prevent irreversible visual deprivation. <br><em>Assessment:</em> Leukocoria (white pupil).
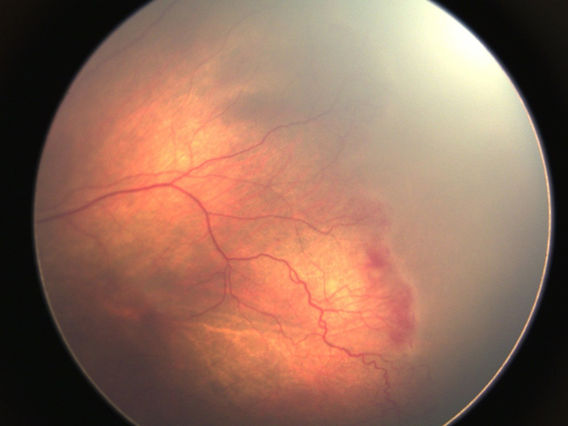
<strong>Retinopathy of Prematurity (ROP):</strong><br>Rapid growth of retinal blood vessels in preemies.<br><em>Risk Factors:</em> High oxygen therapy, low birth weight.<br><em>Nursing:</em> Strict O2 management (maintain lowest target Sat).
Nursing Care for Visual Impairment
<ul><li><strong>Safety:</strong> Keep environment clutter-free. Announce entry/exit. Do not rearrange furniture without orientation.</li><li><strong>Feeding:</strong> Use 'Clock Method' to describe food location on a plate for older children.</li><li><strong>Development:</strong> Promote independence. Encourage tactile toys and Braille early if indicated.</li><li><strong>Communication:</strong> Speak before touching used specifically for invasive procedures.</li></ul>
Acute Otitis Media (AOM)
<strong>Pathophysiology:</strong> Fluid accumulation in the middle ear + infection (bacterial/viral).<br><strong>Key Assessment Findings:</strong><br>• Bulging, opaque, red tympanic membrane.<br>• Pus/effusion visbile.<br>• Child pulling at ears, crying, fever.
Managing AOM: Treatment & Pain
Pharmacology
<ul><li><strong>Wait & See:</strong> Often viral. Observe 48-72h if >2yo and non-severe.</li><li><strong>Antibiotics:</strong> Amoxicillin (First line) if <2yo or severe symptoms.</li><li><strong>Analgesics:</strong> Acetaminophen/Ibuprofen are PRIORITY for comfort during sleep/feeding.</li></ul>
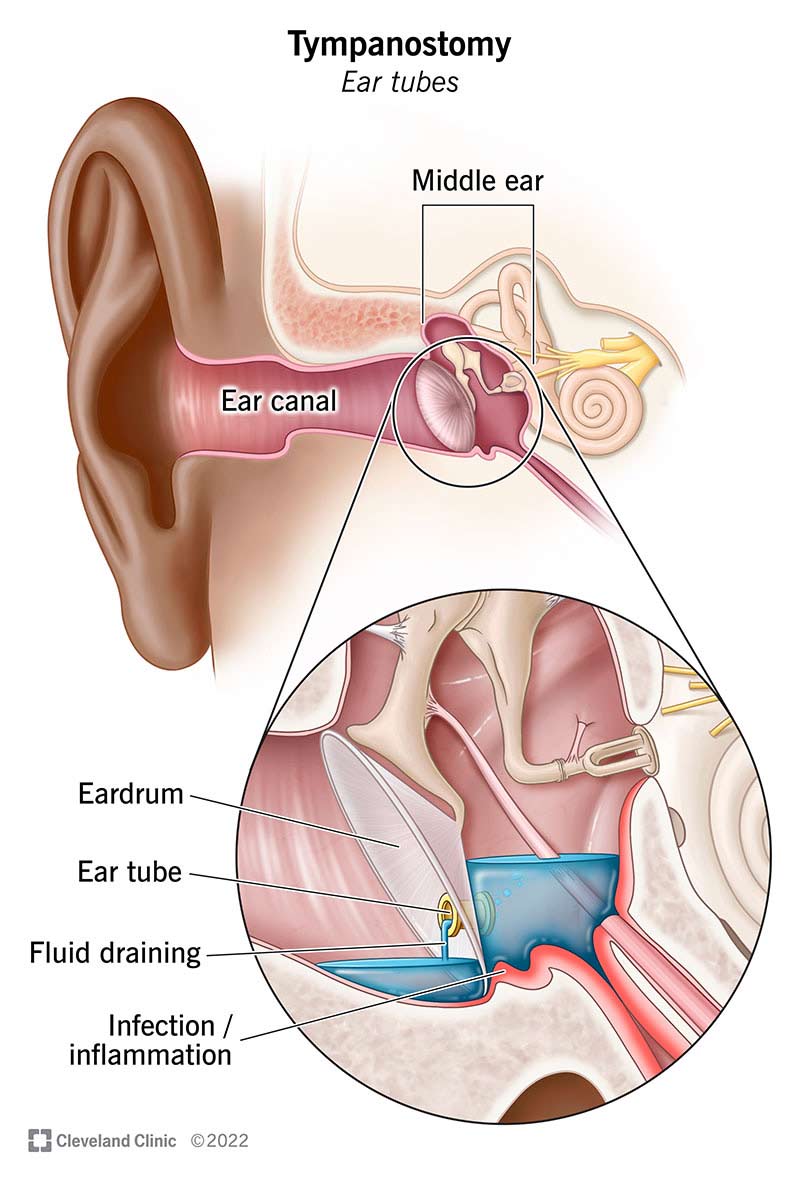
Surgical (Myringotomy)
<ul><li><strong>Tympanostomy Tubes:</strong> For recurrent AOM or effusion >3 months.</li><li><strong>Teaching:</strong> Tubes allow drainage. Keep ears dry (earplugs when swimming).</li><li><strong>Outcome:</strong> Tubes usually fall out spontaneously within 6-12 months.</li></ul>
Hearing Loss & Communication
<ul><li><strong>Conductive vs Sensorineural:</strong> Middle ear issue (AOM) vs Nerve damage (NICU noise, gentamicin).</li><li><strong>Communication Strategies:</strong><br>- Face the child directly.<br>- Verify hearing aid batteries are working.<br>- Use sign language or picture boards if indicated.</li><li><strong>Prevention:</strong> Manage noise levels in NICU/PICU; treat ear infections promptly.</li></ul>
Key Takeaways: Chapter 39
<ul><li><strong>Anatomy:</strong> Horizontal eustachian tubes predispose infants to AOM.</li><li><strong>Pain Mgmt:</strong> AOM pain is severe; manage before procedures or feeding.</li><li><strong>Strabismus/Amblyopia:</strong> Require early intervention (patching) to prevent permanent vision loss.</li><li><strong>Safety:</strong> Priority for visual impairments (orientation) and post-op cataract/tube care.</li><li><strong>Prevention:</strong> Handwashing (conjunctivitis) and finishing antibiotics (resistance).</li></ul>
Questions & Discussion
Open floor for questions about pediatric eye and ear assessments, interventions, or clinical experiences.
Thank you for viewing.
- pediatric-nursing
- sensory-disorders
- otitis-media
- strabismus
- nursing-education
- clinical-pediatrics