



מניעת זיהומים בבתי חולים: מדריך למערכות בריאות
סקירה מקצועית על זיהומים נרכשים בבתי חולים: נתונים בישראל, דרכי מניעה ניהוליות, הגיינת ידיים וניתוח כלכלי של תועלת מול השקעה.
זיהומים נרכשים בבתי החולים
סמינר מלווה פרויקט בניהול מערכות בריאות
מגישים: מוחמד כתכת, דיבה עמאש | מרצה: ד״ר שימי ברדה
ראשי פרקים
הגודל של הבעיה: מספרים ותוצאות בריאותיות
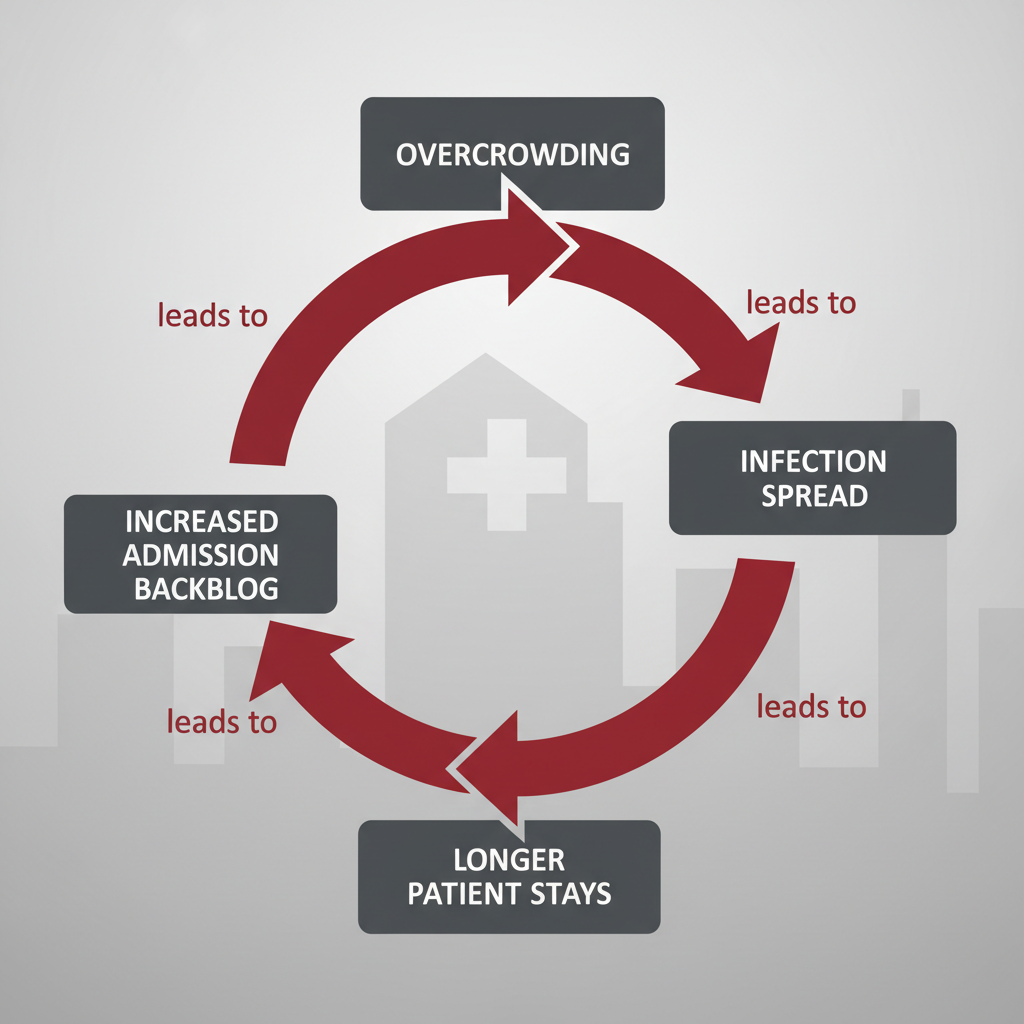
גורמי סיכון בבית החולים: 'מעגל הקסמים'
דרכים ניהוליות למניעת זיהומים
פיקוח, תקנות ודיווח חובה
ניתוח כלכלי: עלויות ותועלת
תוכנית פעולה מורחבת (מודל כלכלי)
סיכום ומסקנות אישיות
היקף הבעיה: נתונים ומחיר כבד
בעולם: 3.5%-12% מהמאושפזים במדינות מפותחות נדבקים. בארה״ב לבדה: כ-75,000 מקרי מוות בשנה (2011). במדינות מתפתחות המספרים מגיעים ל-19.1%.
בישראל: 40,000-100,000 מקרים בשנה. תמותה שנתית של 4,000-6,000 חולים. ניתן למנוע 25%-75% מהמקרים ובכך להציל חיים רבים.
זיהומים בדם וזיהומים באזור הניתוח הם המסוכנים והיקרים ביותר. הסיכון גבוה במיוחד בטיפול נמרץ, ניתוחים, ואוכלוסיות פגיעות.
Major Types of HAIs Tracked
CLABSI: Central Line-Associated Bloodstream Infection
CAUTI: Catheter-Associated Urinary Tract Infection
SSI: Surgical Site Infection
VAP/VAE: Ventilator-Associated Pneumonia/Events
C. difficile: LabID Event (bacterial intestinal infection)
NHSN Surveillance Logic
Infection Window Period (IWP): A 7-day rolling window defined by the first positive diagnostic test ± 3 days.
Repeat Infection Timeframe (RIT): A 14-day period where no new infections of the same type are reported.
Secondary BSI Attribution: Linking a bloodstream infection to a primary site (e.g., UTI source) rather than calling it a CLABSI.
Measuring Quality: Standardized Infection Ratio (SIR)
SIR = Observed Infections / Predicted Infections
Predicted values are adjusted for risk factors (facility size, patient acuity, device utilization).
SIR < 1.0: Better than baseline | SIR > 1.0: Needs Improvement
Prevention Pillar 1: Hand Hygiene
The single most effective way to prevent the spread of infections.
Follow the '5 Moments for Hand Hygiene': Before patient contact, before aseptic task, after body fluid exposure risk, after patient contact, after contact with surroundings.
Use alcohol-based hand rub for routine decontamination; Soap & water for C. diff or visible soiling.
Standard & Contact Precautions
Universal/Standard
Treat all blood and body fluids as potentially infectious. Use gloves and wash hands for all patients.
Transmission-Based
Contact Isolation (Gown + Gloves) for MDROs (MRSA, VRE) and C. difficile. Dedicated equipment for these patients.
Focus Mechanism: Preventing CLABSI
Central Line Insertion Practices (CLIP) Bundle
Maximal sterile barrier precautions (full drape, cap, mask, sterile gown/gloves).
Skin antisepsis with chlorhexidine.
Avoid femoral site if possible (subclavian preferred).
Daily review of line necessity - "Prompt Removal" is key.
Focus Mechanism: Preventing CAUTI
The most effective control measure for Catheter-Associated Urinary Tract Infections is restricting use.
Insert catheters only for appropriate indications (e.g., perioperative use, urinary retention, critical output monitoring).
Maintain a closed drainage system; keep bag below bladder level.
Nurse-driven removal protocols to assess need daily.
Zero Harm: Our Goal
HAIs are preventable. Success relies on accurate surveillance, strict adherence to bundles, and a culture of safety.
Wash hands.
Isolate appropriately.
Remove devices early.
- hospital-acquired-infections
- healthcare-management
- infection-prevention
- patient-safety
- hai-surveillance
- medical-economics
- hand-hygiene