

Understanding RhoGAM: Mechanisms, Timing, and Clinical Use
A clinical guide to Anti-D (RhoGAM) prophylaxis, HDFN prevention, dosing protocols, and laboratory interpretation for Rh-negative pregnancies.
Understanding Anti-D (RhoGAM)
Mechanism of Action, Clinical Indications, and Laboratory Interpretation
Target Audience: Clinicians, Students, and Laboratory Scientist
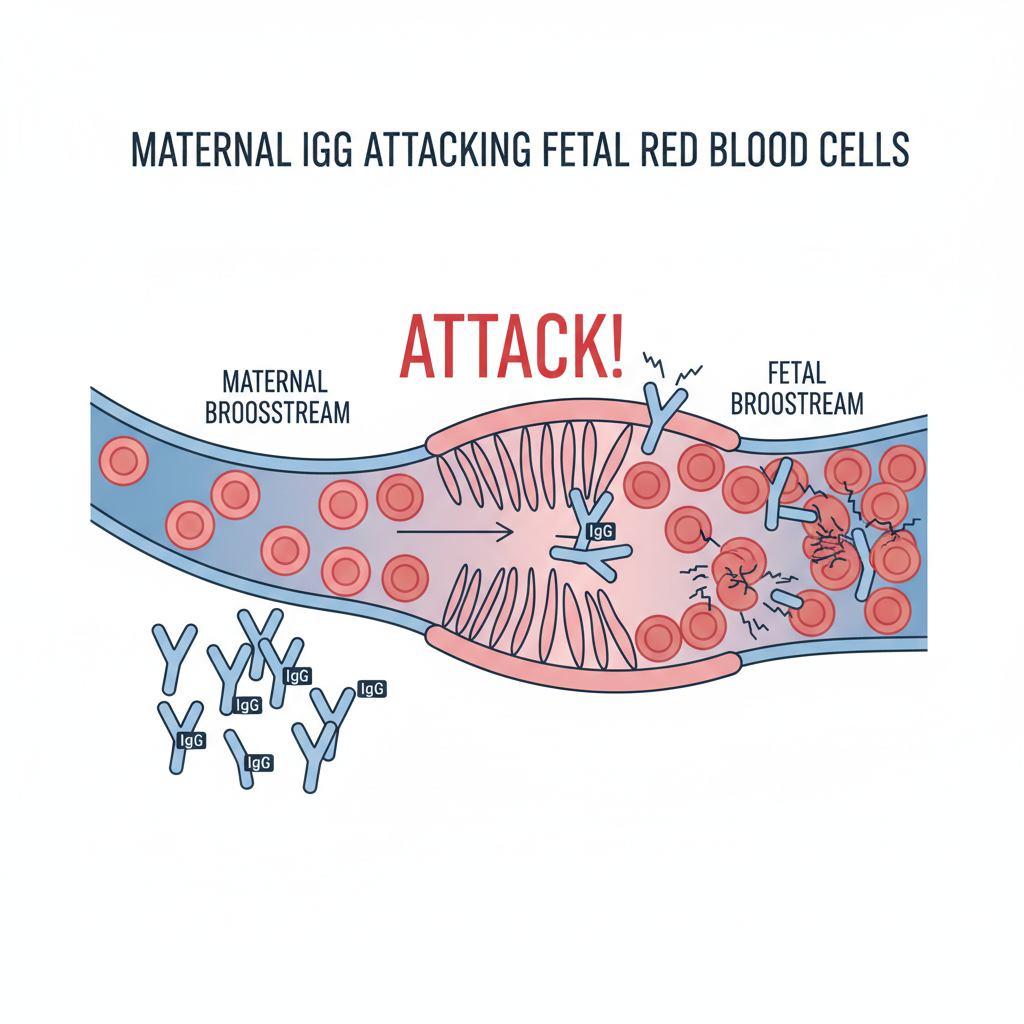
The Clinical Necessity: HDFN
Hemolytic Disease of the Fetus and Newborn (HDFN) occurs when maternal antibodies destroy fetal RBCs.
Rh-negative (D-) mothers exposed to Rh-positive (D+) fetal blood develop active immunity (Alloimmunization).
Subsequent pregnancies with D+ fetuses trigger rapid IgG attack, causing fetal anemia and hydrops.
Mechanism of Action
RhoGAM (Rh Immunoglobulin/RhIg) provides 'Passive Immunity' to suppress the maternal immune response.
<span>1. Clearance:</span> Anti-D binds to D+ fetal cells in maternal circulation.<br/><br/><span>2. Antigen Masking:</span> Blocks D-antigen epitopes (controversial theory).<br/><br/><span>3. Immunoregulation:</span> Downregulates B-cell priming via Fc-gamma receptor stimulation.
Standard Prophylaxis Protocol
Antenatal (Pregnant)
Time: 28 Weeks Gestation<br>Dose: 300 µg (1500 IU)<br>Goal: Protection effectively lasts ~12 weeks to cover third trimester bleeds.
Postpartum (Delivery)
Time: Within 72 Hours<br>Dose: 300 µg minimum<br>Req: Only if baby is Rh Positive (D+). <br>Note: Can be given up to 28 days post-delivery if missed.
Dosing Logic: The 300µg Standard
One standard vial (300µg) suppresses immunity for up to 15 mL of Rh+ Red Blood Cells (approx. 30 mL whole blood).
Indications: Sensitizing Events
Administer Anti-D immediately after any event posing a risk of fetomaternal hemorrhage.
<ul><li>Miscarriage / Threatened Abortion / Ectopic Pregnancy</li><li>Amniocentesis or CVS (Invasive procedures)</li><li>Abdominal Trauma (Car accident, falls)</li><li>External Cephalic Version (ECV)</li><li>Intrauterine Fetal Demise (IUFD)</li></ul>
Quantifying the Bleed: FMH Testing
1. Rosette Test (Screen)
Qualitative test. Rh+ fetal cells form 'rosettes' around anti-D reagent. If positive, signifies a bleed >10 mL. Requires follow-up.
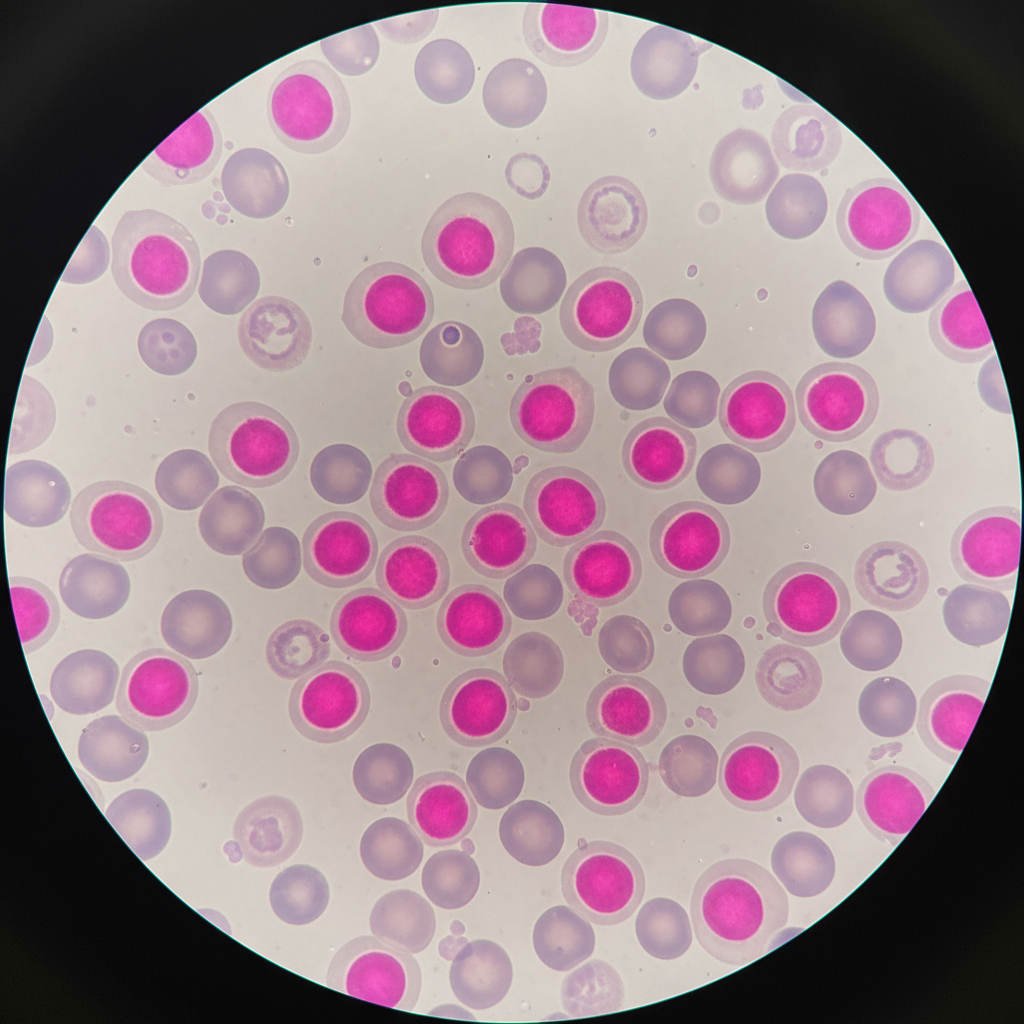
2. Kleihauer-Betke (Quant)
Quantitative acid elution test. Fetal Hgb (HbF) resists acid elution and stains dark pink; Maternal cells appear as 'ghost' cells. Determines exact # of vials needed.
Lab Interpretation: Passive vs. Active Anti-D
A positive antibody screen for Anti-D is EXPECTED after RhoGAM administration.
<b>Passively Acquired Anti-D</b><br>History of recent RhoGAM.<br>Titer is usually low (< 4).<br>No rising titer over time.
<b>Active Allo-Anti-D (Sensitization)</b><br>Immune system response.<br>Titers can be very high (> 16).<br>History of previous sensitization.
Contraindications & Exclusions
<ul><li><b>Rh Positive Females:</b> Do not possess the risk phenotype.</li><li><b>Previously Sensitized:</b> If a woman already has active anti-D alloantibodies, RhoGAM is ineffective (cannot reverse sensitization).</li><li><b>Rh Negative Baby:</b> No D antigen exposure occurred.</li></ul>
Key Takeaways
<ul><li><b>Goal:</b> Prevent active alloimmunization to D antigen.</li><li><b>Timing:</b> Routine at 28 weeks & within 72 hrs postpartum.</li><li><b>Dosing:</b> Standard 300µg covers 15mL fetal RBCs.</li><li><b>Testing:</b> Always screen for bleed volume (FMH) if suspicious.</li><li><b>Lab:</b> Expect positive antibody screens post-administration.</li></ul>
Questions?
- rhogam
- anti-d
- obstetrics
- hematology
- pregnancy-care
- blood-bank
- alloimmunization