



Nuclear Medicine & Radiopharmaceuticals Investment Thesis
Explore the growth of theranostics and nuclear medicine. Strategic deeper-dive into market structure, radiopharmaceutical supply chains, and clinical ROI.
INVESTMENT COMMITTEE PRESENTATION
NUCLEAR MEDICINE
A Comprehensive Strategic & Investment Overview
Technology · Radiopharmaceuticals · Theranostics · Market Structure · Investment Thesis
CONFIDENTIAL — FOR AUTHORIZED RECIPIENTS ONLY
~$17B
Global Market 2024
~15%
Annual Growth Rate (CAGR)
111
PET Scanners in Brazil
8 Sections
Strategic Deep-Dive
May 2026
AGENDA
Presentation Overview
01
What Is Nuclear Medicine
Technical Foundations & Historical Context
02
Radiopharmaceuticals
Isotopes, Mechanism & Supply Chain
03
Clinical Applications & Theranostics
Precision Oncology & Targeted Therapy
04
Industry Structure
Value Chain & Market Economics
05
Suppliers & Production
Cyclotrons, GMP & Logistics
06
Service Providers in Brazil
Business Models & Market Dynamics
07
PET-CT Distribution in Brazil
Geographic Access & Expansion
08
Growth Outlook & Investment Thesis
Drivers, Pipeline & Opportunities
CONFIDENTIAL
Nuclear Medicine | Investment Committee
SECTION 01
What Is
Nuclear Medicine
From Historical Origins to Molecular Imaging
Historical Timeline
Technology vs. Traditional Radiology
PET-CT & SPECT Principles
Clinical Foundations
CONFIDENTIAL
Nuclear Medicine | Investment Committee
SECTION 01 — WHAT IS NUCLEAR MEDICINE
Nuclear Medicine Was Born From Physics — And Is Now Transforming Oncology
A century of scientific breakthroughs converging at the intersection of biology, chemistry, and physics
1896
Discovery of Radioactivity
(Becquerel & Curie)
1934
Artificial Radioactivity
(Joliot-Curie)
1946
First Therapeutic Use
of I-131 (thyroid cancer)
1950s
Technetium-99m
Development phase
1973
First PET Scanner
Prototype (Phelps & Hoffman)
1990s
FDG-PET Clinical Use
Enters standard for oncology
2000s
PET-CT Hybrid Imaging
Becomes standard practice
2013
Lutathera (Lu-177)
Phase III trials begin
2022
Pluvicto FDA Approval
For prostate cancer (Novartis)
2024+
Radioligand Therapy
Pipeline explosion
Nuclear medicine has evolved from diagnostic tool to precision therapeutic platform — a structural shift driving its emergence as a high-growth investment category.
CONFIDENTIAL
03
SECTION 01 — WHAT IS NUCLEAR MEDICINE
Nuclear Medicine Sees What Other Imaging Cannot — Function, Not Just Anatomy
CT SCAN
Anatomical Imaging
X-ray attenuation through tissue
Structure, density, size
Fast, widely available
Cannot show metabolic activity
Low-Medium
MRI
Anatomical + Soft Tissue
Magnetic resonance of hydrogen atoms
Tissue contrast, structure
Excellent soft tissue detail
No functional/metabolic data
High
PET-CT / Nuclear Medicine
FUNCTIONAL + Metabolic Imaging
Radiotracer uptake by active cells
Metabolic activity, receptor expression, cell function
Detects disease EARLIER, guides therapy
Requires radiopharmaceutical supply
Premium
Precision Medicine Standard
While CT and MRI reveal WHERE disease is located, nuclear medicine reveals HOW disease is behaving at the cellular level — enabling earlier detection and personalized treatment decisions.
SECTION 01 — HOW IT WORKS
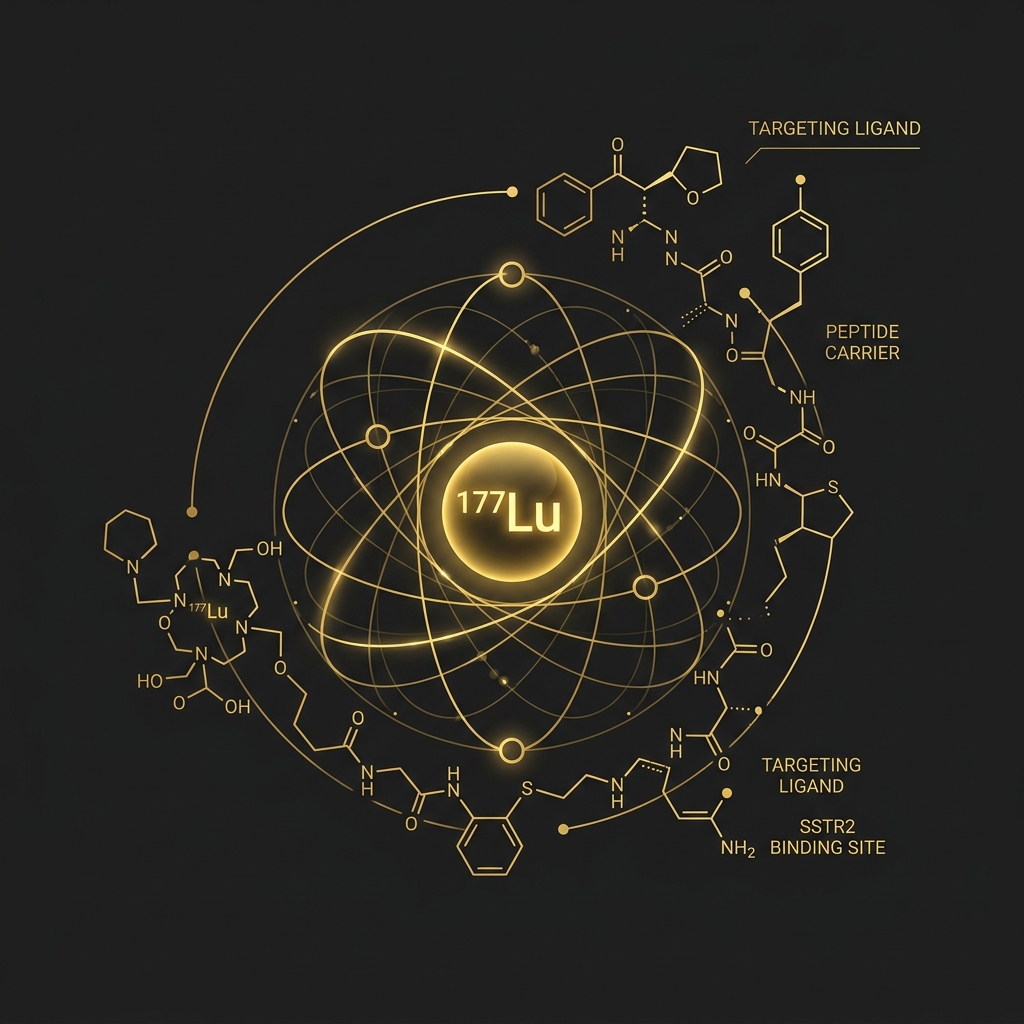
How Nuclear Medicine Works — A Molecular Targeting System
Isotope Production
Radioactive isotopes produced in cyclotron or nuclear reactor (e.g., F-18, Ga-68, Lu-177)
Half-life: minutes to days
Radiopharmaceutical Synthesis
Isotope is bonded to a biological carrier molecule targeting specific receptors or metabolic pathways
Administration to Patient
Injected intravenously; the active compound travels safely through the bloodstream to reach target tissue
Molecular Targeting
Radiopharmaceutical accumulates in target cells (e.g., tumors), strictly guided by binding biological affinity
Imaging / Therapy
PET-CT or SPECT scanner detects gamma rays emitted → creates an exact functional image
Beta or alpha particle emissions selectively destroy the target cells locally while sparing healthy tissue
The same molecular targeting mechanism enables both diagnosis AND treatment — this is the foundation of Theranostics, the fastest-growing segment of nuclear medicine.
SECTION 02
Radiopharmaceuticals
The Critical Infrastructure Behind Nuclear Medicine
Mechanism of Action & Isotope Classes
Diagnostic vs. Therapeutic Applications
Half-Life Dynamics & Logistics
Key Isotopes: FDG, Ga-68, Lu-177, Tc-99m
CONFIDENTIAL — FOR AUTHORIZED RECIPIENTS ONLY
SECTION 02 — RADIOPHARMACEUTICALS
Radiopharmaceuticals Are Purpose-Built Molecular Agents — Each Designed for a Specific Clinical Mission
Isotope
Type
Half-Life
Production Source
Primary Clinical Use
Strategic Notes
FDG (F-18)
Diagnostic
110 min
Cyclotron
Oncology: metabolic tumor imaging (PET-CT)
Most widely used PET tracer globally; ~$1B+ market
Technetium-99m
Diagnostic
6 hours
Generator (Mo-99)
Cardiology, bone, thyroid SPECT imaging
Highest volume isotope worldwide; ~30M procedures/year
Gallium-68
Diagnostic
68 min
Cyclotron or Generator
Neuroendocrine tumors, PSMA prostate cancer
Fastest growing diagnostic tracer; replacing older tracers
Lutetium-177
Therapeutic
6.7 days
Reactor
NETs, Prostate cancer (PSMA); Pluvicto (Novartis)
Blockbuster therapeutic; $1.4B revenue 2024 for Pluvicto alone
Iodine-131
Therapeutic
8 days
Reactor
Thyroid cancer, hyperthyroidism
Oldest therapeutic isotope; still widely used
Short half-lives create critical logistics dependencies — a defining competitive moat
Therapeutic isotopes command 10-20x higher revenue per dose than diagnostics
Supply chain mastery is a strategic advantage in this market
CONFIDENTIAL — FOR AUTHORIZED RECIPIENTS ONLY
02
SECTION 02 — HALF-LIFE & LOGISTICS
Half-Life Is the Invisible Hand Governing the Entire Radiopharmaceutical Supply Chain
Radioactive Decay Profiles by Isotope
From Production to Patient: The Race Against Decay
Isotope Produced at Cyclotron / Reactor
Quality Control & Synthesis
~1-2 hrs
Packaging & Labeling
~30 min
Courier Transport
1-4 hrs
Dose Preparation at Nuclear Pharmacy
~30 min
PATIENT ADMINISTRATION
<strong>For F-18:</strong> total window = ~8 half-lives max
<strong>Warning:</strong> Any supply disruption = appointment cancellation
Half-life constraints create structural moats: only operators with local production or optimized logistics infrastructure can reliably serve clinical demand — a key competitive differentiator.
CONFIDENTIAL — FOR AUTHORIZED RECIPIENTS ONLY
Q2 DEEP-DIVE STRATEGY
SECTION 03
Clinical Applications
& Theranostics
Precision Oncology's Most Powerful Emerging Paradigm
Diagnostic & Therapeutic Applications
The Theranostics Revolution
Prostate Cancer & NETs Case Studies
Economic Comparison vs. Standard of Care
CONFIDENTIAL — FOR AUTHORIZED RECIPIENTS ONLY
SECTION 03 — THERANOSTICS
Theranostics: The Same Molecule That Finds the Cancer Also Destroys It
Theranostics merges THERApeutics + diagNOSTICS — a paradigm shift from systemic to precision-targeted treatment
Ga-68 PSMA PET-CT Scan
LOCATES receptor-expressing cancer cells
Confirms PSMA expression → Patient eligible for therapy
Lu-177 PSMA Therapy
DELIVERS lethal radiation to same receptor
Targeted cell destruction, minimal collateral damage
One Target. One Molecule. Two Powers.
The PSMA receptor serves as both the GPS and the delivery address
1. PROSTATE CANCER (PSMA)
Lu-177 PSMA; Pluvicto approved FDA 2022
2. NEUROENDOCRINE TUMORS (SSTR)
Lu-177 DOTATATE; Lutathera approved
3. THYROID CANCER
I-131; classic theranostic pair with diagnostic I-123
VISION Trial
Pluvicto + std care → 38% reduction in death vs std care alone
NETTER-1 Trial
Lutathera → 79% disease control rate in NETs
First major oncology approvals based on theranostic pairs
Theranostics represents the first true implementation of precision medicine at scale — combining diagnostic accuracy with therapeutic precision in a single biological framework.
SECTION 03 — ECONOMIC & CLINICAL COMPARISON
Theranostics Outperforms Conventional Oncology on Every Dimension That Matters
Theranostics (Lu-177 PSMA)
Chemotherapy (Cabazitaxel)
Immunotherapy (Pembrolizumab)
Hormone Therapy (Enzalutamide)
Overall Survival Benefit
✓✓✓ Best
✓ Modest
✓✓ Moderate
✓✓ Moderate
Radiographic PFS
8.7 months gain
2.8 months
4.2 months
5.6 months
Adverse Effects
Targeted, low systemic tox
High systemic toxicity
Immune-related AEs
Fatigue, falls
Quality of Life
↑ Preserved/Improved
↓ Significantly impacted
Variable
Moderate impact
Response Rate (PSA)
~80%
~35%
~25%
~55%
Cost per Cycle (USD)
~$42,000
~$8,000
~$15,000
~$5,000
Total Course Cost (USD)
~$200,000
~$50,000
~$120,000
~$60,000
Value per Outcome
HIGH (vs standard)
Medium
Medium-High
Medium
Despite higher per-cycle cost, theranostics delivers superior outcomes per dollar spent — and reduced hospitalization costs narrow the net cost differential significantly.
Source: VISION Trial (NEJM, 2021); NETTER-1 Trial; comparative oncology analyses
Reimbursement expansion by payers is accelerating as health-economic evidence accumulates
SECTION 03 — CLINICAL APPLICATIONS
Nuclear Medicine Serves Four Major Specialties — Oncology Dominates But Cardiology and Neurology Are Fast-Growing
Oncology
~65% of procedures
<div style="display: flex; gap: 10px; margin-bottom: 8px; align-items: flex-start;"><div style="color: #C9A84C; font-size: 18px; line-height: 1.2;">•</div><div style="line-height: 1.3;">PET-CT staging & restaging</div></div><div style="display: flex; gap: 10px; margin-bottom: 8px; align-items: flex-start;"><div style="color: #C9A84C; font-size: 18px; line-height: 1.2;">•</div><div style="line-height: 1.3;">Response assessment</div></div><div style="display: flex; gap: 10px; margin-bottom: 8px; align-items: flex-start;"><div style="color: #C9A84C; font-size: 18px; line-height: 1.2;">•</div><div style="line-height: 1.3;">Theranostics (PSMA, SSTR)</div></div><div style="display: flex; gap: 10px; margin-bottom: 8px; align-items: flex-start;"><div style="color: #C9A84C; font-size: 18px; line-height: 1.2;">•</div><div style="line-height: 1.3;">Bone metastases detection</div></div>
FDG, Ga-68, Lu-177, Ra-223
Fastest growing due to theranostics expansion
Cardiology
~20% of procedures
<div style="display: flex; gap: 10px; margin-bottom: 8px; align-items: flex-start;"><div style="color: #C9A84C; font-size: 18px; line-height: 1.2;">•</div><div style="line-height: 1.3;">Myocardial perfusion imaging</div></div><div style="display: flex; gap: 10px; margin-bottom: 8px; align-items: flex-start;"><div style="color: #C9A84C; font-size: 18px; line-height: 1.2;">•</div><div style="line-height: 1.3;">Viability assessment</div></div><div style="display: flex; gap: 10px; margin-bottom: 8px; align-items: flex-start;"><div style="color: #C9A84C; font-size: 18px; line-height: 1.2;">•</div><div style="line-height: 1.3;">Cardiac sarcoidosis</div></div><div style="display: flex; gap: 10px; margin-bottom: 8px; align-items: flex-start;"><div style="color: #C9A84C; font-size: 18px; line-height: 1.2;">•</div><div style="line-height: 1.3;">Amyloidosis</div></div>
Tc-99m, Thallium-201, F-18
Stable demand, digital SPECT driving efficiency
Neurology
~10% of procedures
<div style="display: flex; gap: 10px; margin-bottom: 8px; align-items: flex-start;"><div style="color: #C9A84C; font-size: 18px; line-height: 1.2;">•</div><div style="line-height: 1.3;">Alzheimer's / dementia (Amyloid PET)</div></div><div style="display: flex; gap: 10px; margin-bottom: 8px; align-items: flex-start;"><div style="color: #C9A84C; font-size: 18px; line-height: 1.2;">•</div><div style="line-height: 1.3;">Parkinson's disease</div></div><div style="display: flex; gap: 10px; margin-bottom: 8px; align-items: flex-start;"><div style="color: #C9A84C; font-size: 18px; line-height: 1.2;">•</div><div style="line-height: 1.3;">Epilepsy focus localization</div></div><div style="display: flex; gap: 10px; margin-bottom: 8px; align-items: flex-start;"><div style="color: #C9A84C; font-size: 18px; line-height: 1.2;">•</div><div style="line-height: 1.3;">Brain tumors</div></div>
F-18 (amyloid tracers), DaTscan (I-123)
High growth potential with aging population
Endocrinology
~5% of procedures
<div style="display: flex; gap: 10px; margin-bottom: 8px; align-items: flex-start;"><div style="color: #C9A84C; font-size: 18px; line-height: 1.2;">•</div><div style="line-height: 1.3;">Thyroid cancer</div></div><div style="display: flex; gap: 10px; margin-bottom: 8px; align-items: flex-start;"><div style="color: #C9A84C; font-size: 18px; line-height: 1.2;">•</div><div style="line-height: 1.3;">Hyperthyroidism</div></div><div style="display: flex; gap: 10px; margin-bottom: 8px; align-items: flex-start;"><div style="color: #C9A84C; font-size: 18px; line-height: 1.2;">•</div><div style="line-height: 1.3;">Parathyroid adenoma</div></div><div style="display: flex; gap: 10px; margin-bottom: 8px; align-items: flex-start;"><div style="color: #C9A84C; font-size: 18px; line-height: 1.2;">•</div><div style="line-height: 1.3;">Adrenal imaging</div></div>
I-131, I-123, Tc-99m
Foundational segment, highly established
The clinical breadth of nuclear medicine — spanning oncology to neurology — provides structural revenue diversification unavailable to single-specialty diagnostic modalities.
SECTION 04
Industry Structure
Value Chain Economics & Market Organization
End-to-End Sector Value Chain
Service Providers vs. Radiopharmaceutical Suppliers
Revenue Models & Economics
Vertical Integration Dynamics
CONFIDENTIAL — FOR AUTHORIZED RECIPIENTS ONLY
SECTION 04 — VALUE CHAIN
The Nuclear Medicine Value Chain Spans Five Layers — Each With Distinct Economics and Barriers
ISOTOPE PRODUCTION
Nuclear reactors (Mo-99/Tc-99m), Cyclotrons (F-18, Ga-68), Research reactors
Key players: NRU Canada, OPAL Australia, BR2 Belgium, IRR Brazil (IPEN)
Very high capex ($50-500M+), heavily regulated, limited global supply
Barrier to entry: EXTREME
RADIOPHARMACEUTICAL MANUFACTURING
Pharma manufacturers, specialty radiopharmaceutical companies
Brazil: CMR Pharma, R2 Pharma, multinational distributors
High capex, GMP compliance, 24/7 operations
Barrier: VERY HIGH
DISTRIBUTION & LOGISTICS
Cold chain logistics, dose calibration, courier networks
Key constraint: Half-life driven time pressure
Recurring cost, geography-dependent
Barrier: HIGH (specialized infrastructure)
NUCLEAR MEDICINE SERVICES
Hospitals, diagnostic clinics, standalone PET centers
Services: PET-CT, SPECT, dosimetry, therapy administration
High equipment capex ($1-3M per PET-CT), licensed physicians required
Barrier: HIGH
CLINICAL INTEGRATION
Oncologist referrals, treatment planning, follow-up imaging
Fee-per-service, reimbursement-dependent
Note: Increasing integration with tumor boards
VERTICAL INTEGRATION OPPORTUNITY
Integrated players (like Novartis / Advanced Accelerator Applications) span multiple layers.
Vertically integrated operators capturing both radiopharmaceutical production and service delivery command superior margins and supply security — the primary consolidation thesis in this sector.
SECTION 05
Suppliers &
Radiopharmaceutical Production
Critical Infrastructure, Regulatory Complexity & Competitive Moats
Cyclotron Technology & Radiochemistry
GMP Compliance & Regulatory Requirements
ANVISA & CNEN Regulatory Framework
Barriers to Entry & Capital Requirements
CONFIDENTIAL — FOR AUTHORIZED RECIPIENTS ONLY
SECTION 05 — PRODUCTION INFRASTRUCTURE
Radiopharmaceutical Production Is One of Healthcare's Most Regulated and Capital-Intensive Operations
The Production Process
Target Material Preparation
O-18 enriched water for F-18 isotopes<br>Solid metal targets for Ga-68 processing
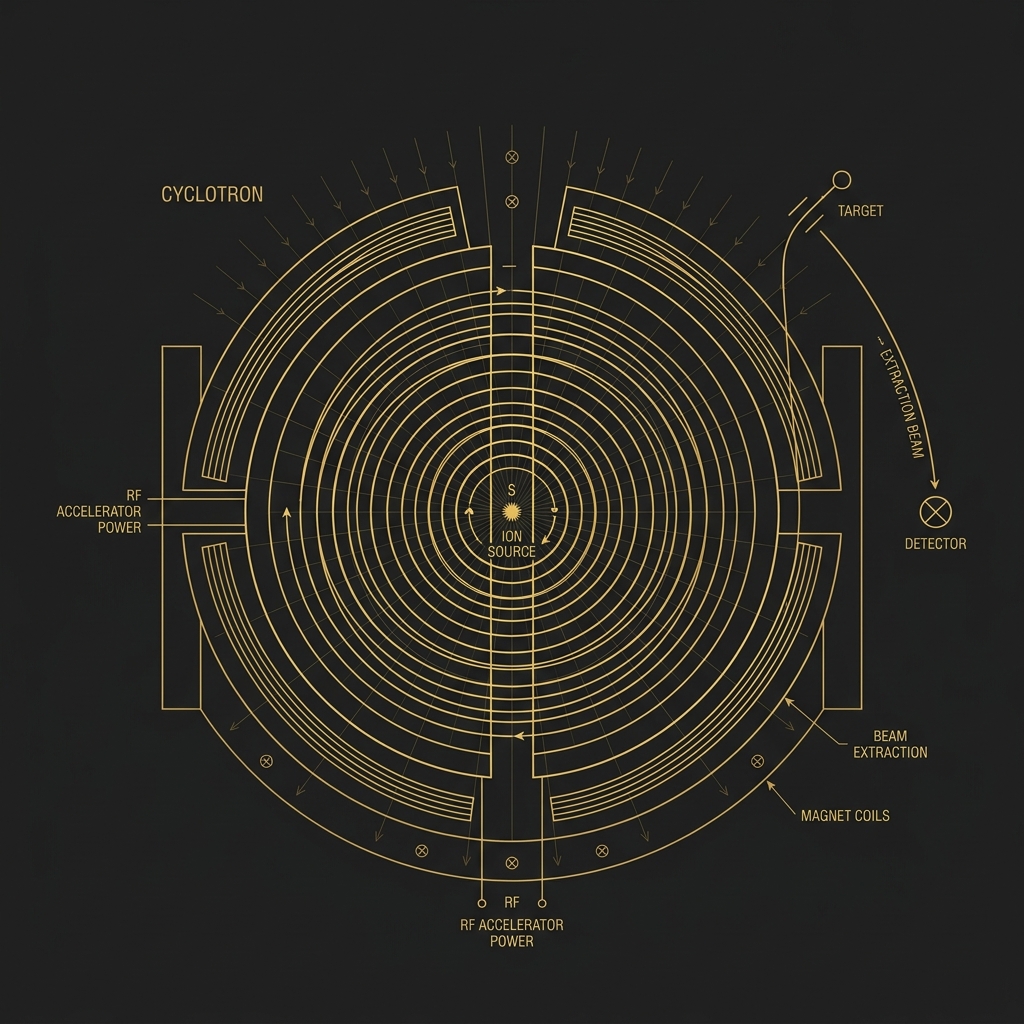
Cyclotron Bombardment
Proton beam (16-18 MeV) bombards target<br>Nuclear reaction produces radioisotope<br><span style='color:#C9A84C; font-weight:600; font-size:14px; margin-top:4px; display:inline-block;'>Time: ~60-90 minutes</span>
Hot Cell Processing
Lead-shielded, remote-controlled synthesis<br>Isotope bonded to precise biological vector
Quality Control (QC)
Sterility, radionuclidic & chemical purity tests<br>Strict Good Manufacturing Practice (GMP)<br><span style='color:#C9A84C; font-weight:600; font-size:14px; margin-top:4px; display:inline-block;'>Time: ~30-60 minutes</span>
Dispensing & Packaging
Unit doses prepared for specific patient needs<br>Loaded into transport vials & shielded syringes<br><span style='color:#C9A84C; font-weight:600; font-size:14px; margin-top:4px; display:inline-block;'>Time: ~30 minutes</span>
Dispatch & Logistics
Temperature-controlled certified delivery<br>Radiation-labeled packaging (IAEA standards)
Barriers to Entry Framework
Initial Capex (cyclotron + hot cells)
●●●●●
$3-8M USD
GMP Facility Construction
●●●●●
$2-5M USD
ANVISA Pharmaceutical License
●●●●○
18-36 months
CNEN Radioactive Materials Lic.
●●●●●
Strict standards
Qualified Technical Staff
●●●●○
Scarce locally
24/7 Operations Requirement
●●●●○
High fixed OPEX
Supply Chain Dependencies
●●●●○
Critical agreements
Geographic Reach Constraints
●●●●●
Half-life limits
CAPEX SUMMARY
Cyclotron (IBA Cyclone 18 MeV)
~$3.5-5M
Hot cell suite
~$1.5-2M
GMP lab infrastructure
~$1-2M
Licensing & validation
~$0.5-1M
Total Minimum Capex
~$7-12M USD
Capital requirements, regulatory timelines, and specialized technical expertise combine to create near-impenetrable barriers — protecting incumbents and limiting competitive entry.
SECTION 05 — BRAZIL SUPPLIER LANDSCAPE
Brazil's Radiopharmaceutical Landscape Is Concentrated, Strategically Critical, and Poised for Consolidation
PUBLIC / INSTITUTIONAL
IPEN / CNEN
Brazil's national nuclear research institute
Produces Mo-99/Tc-99m generators nationally
Cyclotron facility in São Paulo
Critical national infrastructure
Strategic importance: National supply security
PRIVATE SECTOR
CMR Pharma
Leading private Brazilian company
Multiple cyclotron sites nationally
FDG, Ga-68, and other PET tracers
Nuclear pharmacy network
Serving major PET centers across Brazil
PRIVATE SECTOR
R2 Pharma
Growing Brazilian radiopharmaceutical supplier
Cyclotron-based production
Cold kit portfolio (Tc-99m, Ga-68, Lu-177)
Turnkey on-site programs for hospitals
CNEN-approved Ga-68 program
Nuclear pharmacy services
INTERNATIONAL
International Players
Novartis / AAA (Advanced Accelerator) — Pluvicto import
Curium Pharma (European supplier)
GE HealthCare (Tc-99m generators imported)
Limited direct presence; mostly via distributors
The Brazilian radiopharmaceutical supply market is oligopolistic — dominated by 2-3 players with cyclotron infrastructure. This concentration creates both risk (supply disruption) and opportunity (platform M&A).
SECTION 06
Service Providers
in Brazil
Business Models, Economics & Competitive Dynamics
Public vs. Private vs. Independent Models
Cost Structures & Revenue Models
Capital Intensity & Workforce Requirements
Consolidation & Expansion Opportunities
CONFIDENTIAL — FOR AUTHORIZED RECIPIENTS ONLY
SECTION 06 — SERVICE PROVIDER MODELS
Three Distinct Business Models Compete in Brazil's Nuclear Medicine Services Market — Each With Different Economic Profiles
PUBLIC / SUS PROVIDERS
Hospitals universitários, INCA, Santa Casa networks
SUS reimbursement (SIGTAP/AIH)
~R$1,500-2,500 per procedure (SUS)
High (but reimbursement insufficient)
Publicly funded
CLT / public servants
Accessibility, volume
Underfunded, long wait times, equipment outdated
Large underserved patient population
HOSPITAL-BASED / DIAGNOSTIC NETWORKS
Fleury, Dasa, Alliar, Hermes Pardini, Einstein, Sírio-Libanês
ANS reimbursement + private pay
~R$3,500-6,000+ per procedure (private)
Medium-High
$1-3M per PET-CT scanner
Employed nuclear medicine physicians, technologists
Brand, insurance contracts, multidisciplinary integration
High overhead, geographic concentration
CONSOLIDATION TARGETS — scale-driven economics
INDEPENDENT NUCLEAR MEDICINE CLINICS
Specialist standalone nuclear medicine centers
ANS + private pay + direct patient
~R$4,000-8,000+ (premium positioning)
Low-Medium (specialized)
$1.5-3M (owned scanner)
Nuclear medicine physician owner-operators
Specialization, efficiency, patient experience
Single location, no scale, succession risk
ACQUISITION OPPORTUNITY — founder-owned, scalable
Low
Medium
High
Low
Medium-High
High
Low
Very High
Low-Medium
Low
★★★★★
★★★★☆
Hospital-based diagnostic networks offer the ideal combination of scale, insurance contracts, and consolidation potential — while independent clinics represent attractive bolt-on acquisition opportunities.
SECTION 07
PET-CT Distribution
in Brazil
Geographic Inequality, Access Gaps & Expansion Opportunity
Scanner Distribution by Region
International Benchmarking
Supply-Demand Imbalance
Strategic Expansion Thesis
CONFIDENTIAL — FOR AUTHORIZED RECIPIENTS ONLY
SECTION 07 — PET-CT DISTRIBUTION
Brazil Has 111 PET Scanners for 215 Million People —
A Structural Supply Gap That Defines the Investment Opportunity
Regional Distribution in Brazil
International Benchmarking — PET Scanners per Million Population (2024)
75 Scanners
0.84 per million (89M pop)
18 Scanners
0.60 per million (30M pop)
11 Scanners
0.19 per million (57M pop)
4 Scanners
0.25 per million (16M pop)
4 Scanners
0.22 per million (18M pop)
10x below US levels
Brazil's nuclear medicine access is concentrated in 3 metropolitan areas — the remaining 60% of the population remains structurally underserved.
Each new PET center in an underserved region immediately captures suppressed demand — implying above-average utilization and rapid payback.
SECTION 08
Growth Outlook &
Investment Thesis
Structural Tailwinds, Market Sizing & Strategic Opportunities
Global & Brazil Market Growth Projections
Key Structural Growth Drivers
Pipeline & Reimbursement Catalysts
M&A Landscape & Investment Thesis
CONFIDENTIAL — FOR AUTHORIZED RECIPIENTS ONLY
SECTION 08 — MARKET SIZING
Nuclear Medicine Is a ~$17B Global Market Growing at 13-15% CAGR — Driven by Oncology, Theranostics, and an Aging Population
Global Nuclear Medicine Market (USD Billions)
Sources: Grand View Research, MarketsandMarkets, GlobalData, 2024
Market Breakdown by Segment (2024)
The sector exhibits the rare combination of high growth, high barriers to entry, and pricing power — characteristics typically associated with exceptional investment returns.
- nuclear-medicine
- radiopharmaceuticals
- theranostics
- healthcare-investment
- oncology
- market-analysis
- precision-medicine
- biotech