Managing Refractory Diarrhoea in HER2-Positive Breast Cancer
Clinical case study on managing refractory diarrhoea and Clostridioides difficile in breast cancer patients undergoing TCHP-P chemotherapy.
Management of Refractory Diarrhoea in a HER2-Positive Breast Cancer Patient
Oncology Ward Teaching Session
References: UKONS, BC Cancer, Cancer Care Ontario
Background & Baseline GI Vulnerability
Middle aged female, HER2+ Breast Cancer (ER 0%, PR 4%)
Neoadjuvant TCHP-P (Docetaxel, Carboplatin, Phesgo)
Chronic Grade 2 diarrhoea during each cycle
Dose reductions required
Acute Presentation – Day 1
15–20 stools/day
BP 80/47, HR 120–130 (Fast AF)
Temp 38.5°C
AKI Stage 3 (eGFR 12)
WBC 16.7, CRP 403
Initial Management
Aggressive IV fluids
Electrolyte replacement (K+, Mg2+)
IV Ceftazidime (penicillin intolerance)
Cardiac monitoring
AKI and AF resolved
Stabilisation then Deterioration - Day 5
Day 5: WBC 8.5, CRP 135, eGFR 84 Stepped down antibiotics to oral cefalaxin and metronidazole Day 6: WBC rose to 30.8 Stopped cefalaxin, added oral vancomycin and switched metronidazole to IV Day 7: CRP peaked at 295
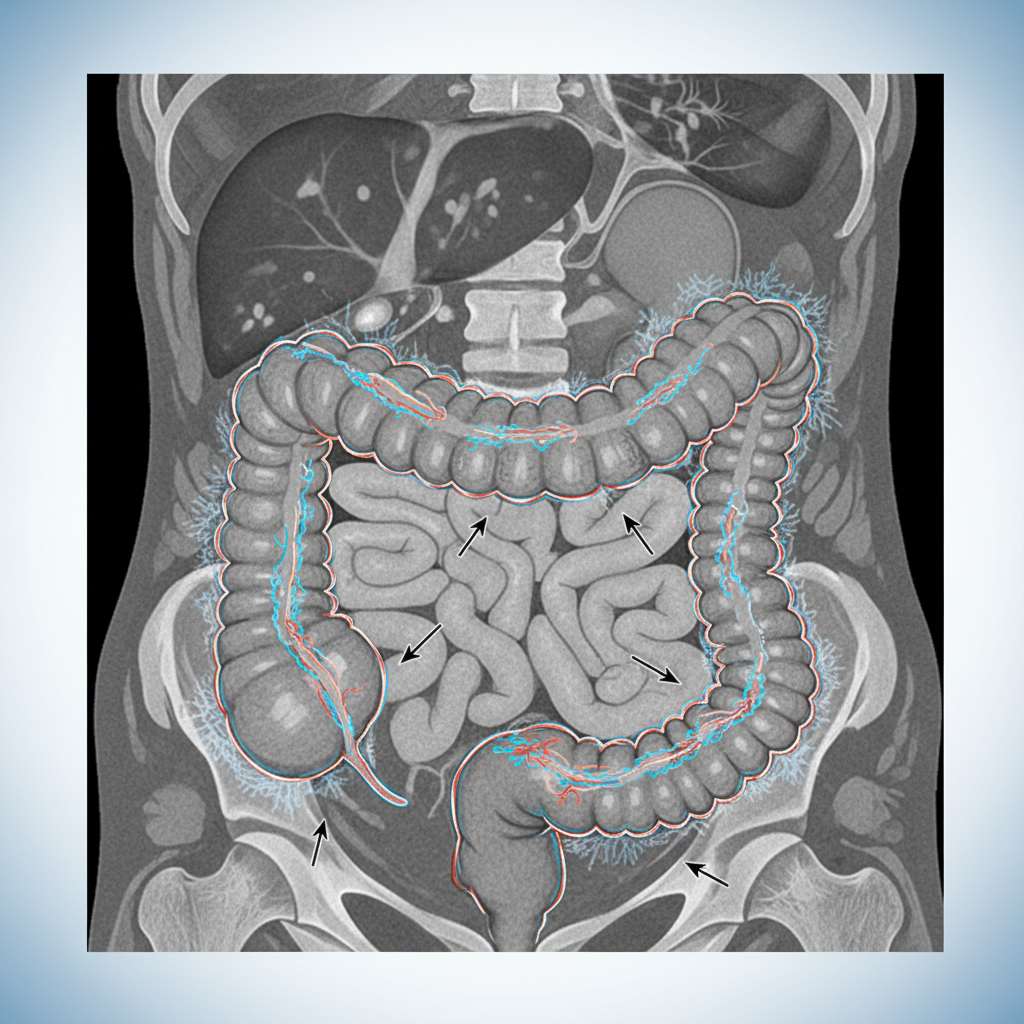
Imaging & Escalation
AXR: colonic thickening, no perforation
CT CAP: diffuse colitis
Started fidaxomicin
Stopped vancomycin and continued with IV metronidazole
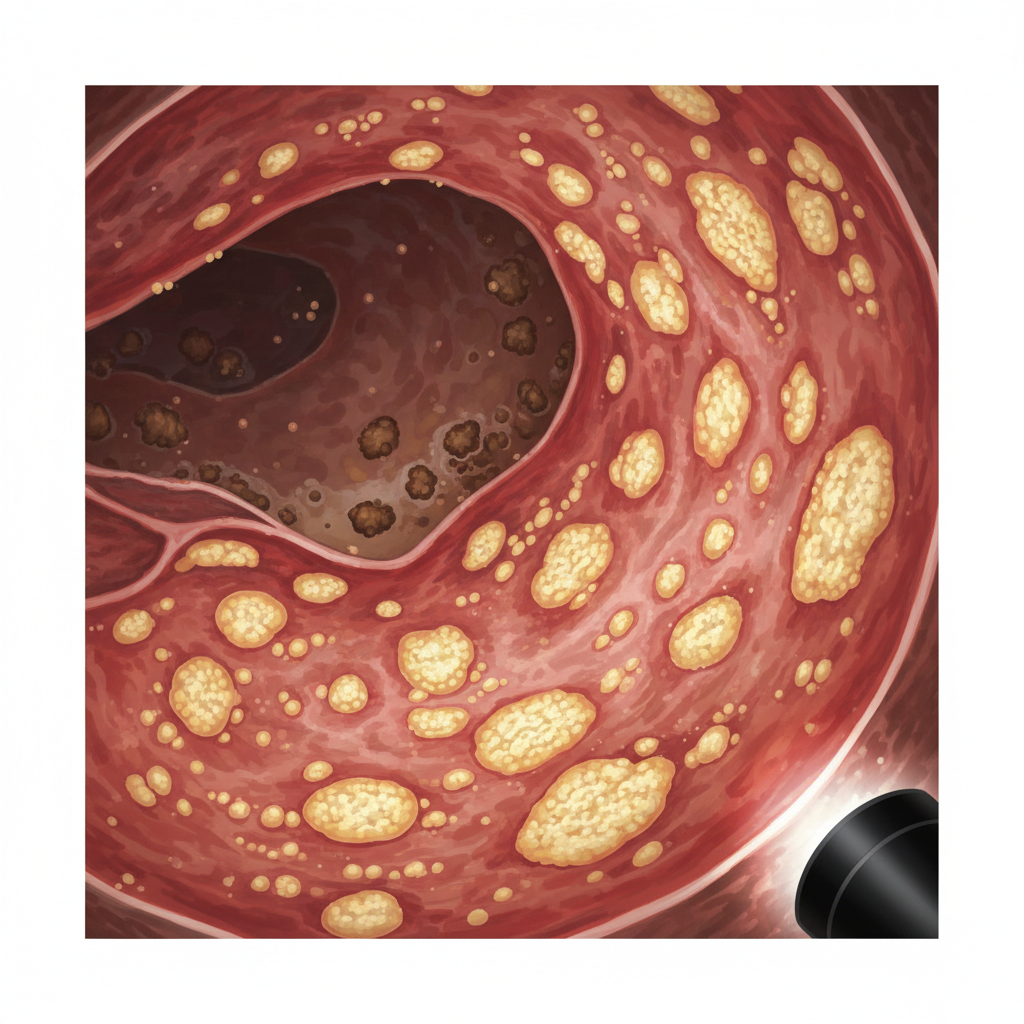
Endoscopic Confirmation
Flexible sigmoidoscopy (9 Jan)
Pseudomembranous colitis
Visual diagnosis supersedes toxin assays
High-volume diarrhoea causes toxin dilution
Antibiotic Strategy Evolution
Fidaxomicin ×12 days
IV metronidazole ×13 days
High-dose oral vancomycin
Extended fidaxomicin taper
BC cancer suggest no FMT in patients with active cancer treatment
Current Status
18–22 stools/day
Refractory hypokalaemia & hypomagnesaemia
Daily IV replacement
Renal function stable (eGFR 84)
Clostridioides difficile (C. diff) infection
• c-diff toxin -ve, PCR +VE, Pseudomembranous colitis<br>• Per BC Cancer / CCO, visual pseudomembranes override negative toxin assays<br>• High-volume secretory diarrhoea → toxin dilution
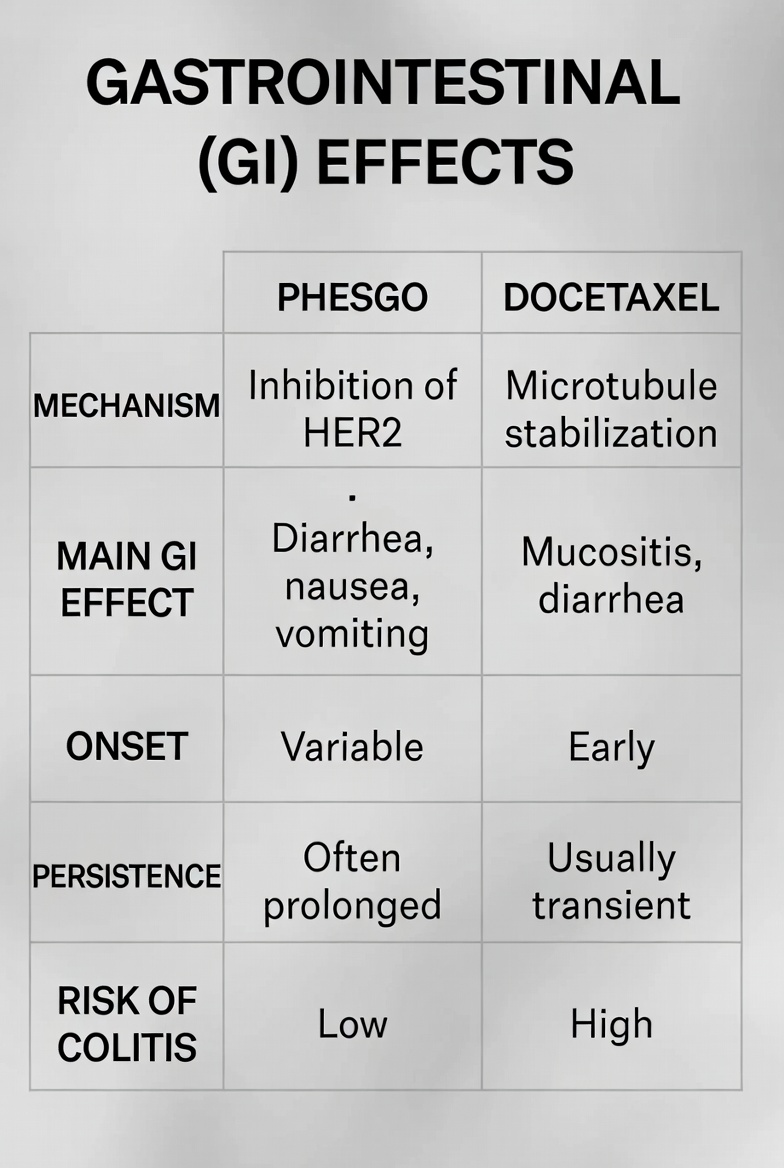
Drug Induced Diarrhea
Phesgo: HER2/EGFR inhibition → impaired mucosal repair
Secretory diarrhoea & electrolyte loss
Docetaxel: crypt cell toxicity & mucositis
Combined 'double-hit' gut injury
Gastrointestinal (GI) Effects
CMV Colitis
CMV IgM weakly positive
CMV PCR pending
Must exclude CMV before escalation
Guideline-supported in oncology patients
Key Learning Points
Persistent diarrhoea ≠ chemotherapy alone
Early infection exclusion critical
CRP may normalise before clinical recovery
Refractory CDI requires MDT approach
Next Steps
Complete fidaxomicin taper
Review CMV PCR result
Continue electrolyte monitoring
GI & Microbiology follow-up
Thank you for your attention
- oncology
- breast-cancer
- chemotherapy-side-effects
- c-diff
- her2-positive
- medical-education
- colitis