



Amniotomy Clinical Guidelines: Techniques & Safety Protocols
Master the artificial rupture of membranes (AROM). Learn aseptic techniques, clinical indications, contraindications, and emergency cord prolapse management.
Artificial Rupture of Membranes (Amniotomy)
Clinical Guidelines, Technique, and Safety Protocols for L&D Providers
Learning Objectives
Identify indications for induction vs. augmentation favoring amniotomy.
Recognize absolute contraindications to prevent catastrophic outcomes.
Demonstrate proper Aseptic Non-Touch Technique (ANTT) during procedure.
Interpret post-procedure fetal heart rate (FHR) changes and amniotic fluid characteristics.
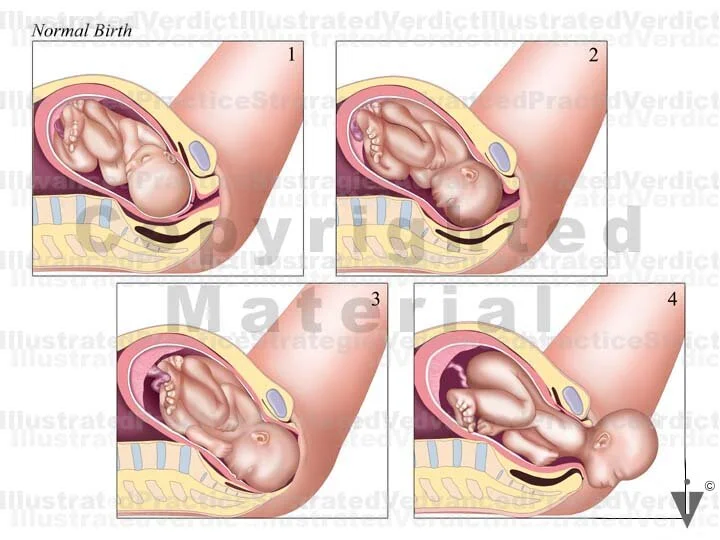
Physiology & Mechanism of Action
Two primary mechanisms: 1. Prostaglandin Release: Rupture increases PGF2α, boosting contractility. 2. Mechanical Pressure: Fetal head applies direct pressure to cervix, stimulating Ferguson reflex.
Clinical Indications
Induction of Labor
Initiate labor (+ oxytocin). Early amniotomy (<4cm) may shorten duration.
Augmentation
Fix arrested active phase (no change >4h) by increasing intensity.
Internal Monitoring
Access for FSE or IUPC placement.
Absolute Contraindications
Vasa Previa
Unengaged / High Fetal Station
Funic (Cord) Presentation
Active Genital Herpes (HSV)
Unknown Fetal Presentation
Clinical Evidence: Impact on Labor Duration (Induction)
Reduction in delivery time with early amniotomy in induction.
Pre-Procedure Safety Checklist
Verify Presentation: Must be Cephalic/Vertex.
Check Station: Head engaged/applied (Ideally ≤ -1).
Fetal Status: Reassuring FHR baseline (prev. 20m).
Consent: Risks (prolapse, infection) discussed.
Equipment & ANTT Protocol
Required Supplies
• Sterile Gloves • Amnihook (or Amnicot for difficult access) • Sterile Lubricant • Absorbent Pads • Fetal Monitor
Aseptic Non-Touch Technique (ANTT)
Minimize chorioamnionitis risk. Maintain sterile field. Avoid touching sharp tip to unsterile surfaces. Limit exams after rupture.
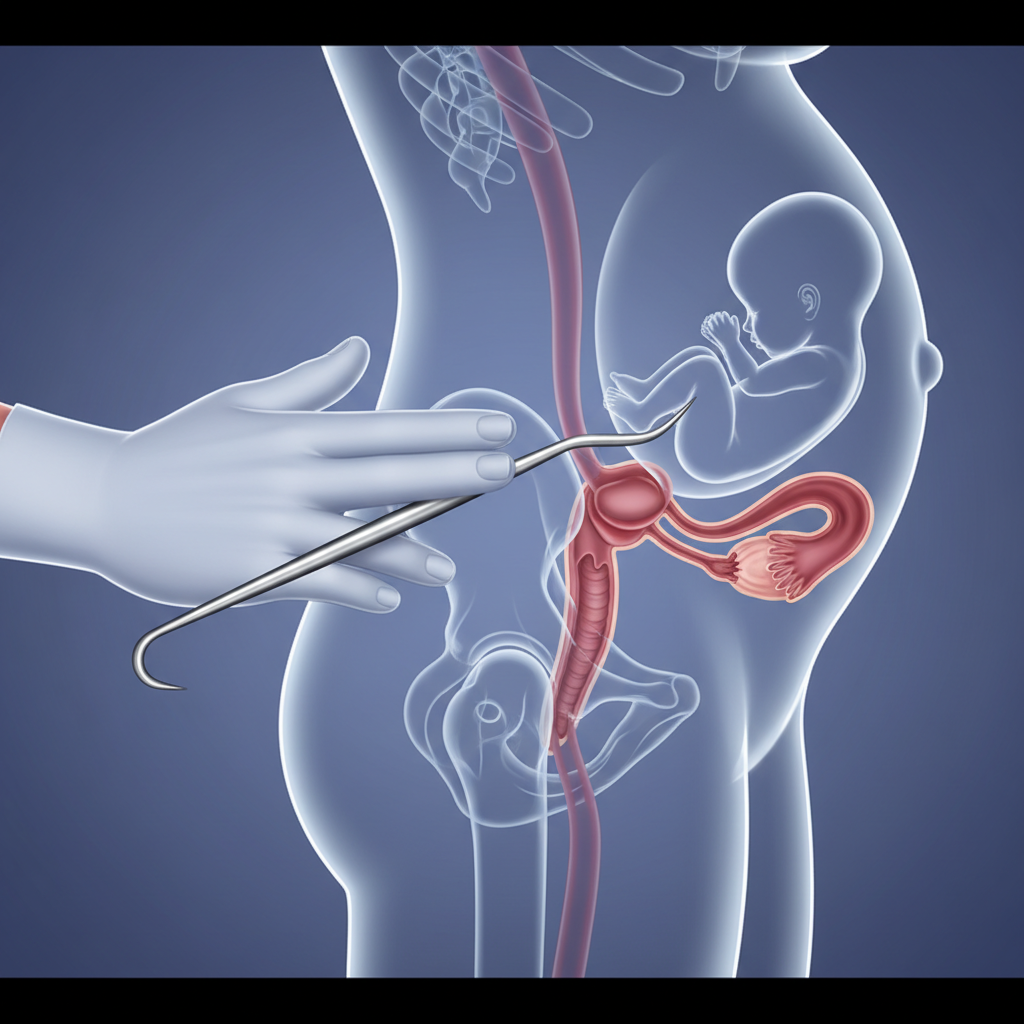
Technique: Step-by-Step
1. Assess & Position: Confirm dilation/station via SVE. Keep known finger position.
2. Insert Hook: Slide Amnihook along palm to protect maternal tissues.
3. Rupture: Snag bag & pull gently between contractions.
4. Control Fluid: Maintain finger position to prevent cord prolapse.
Post-Procedure Assessment
Observe "C.O.A.T"
COLOR: Clear, Meconium (green), Bloody.
ODOR: Earthy (normal) vs Foul (infection).
AMOUNT: Scant, Moderate, or Large.
TIME: Document exact rupture time.
CRITICAL: Check FHR immediately for variables or bradycardia (prolapse).
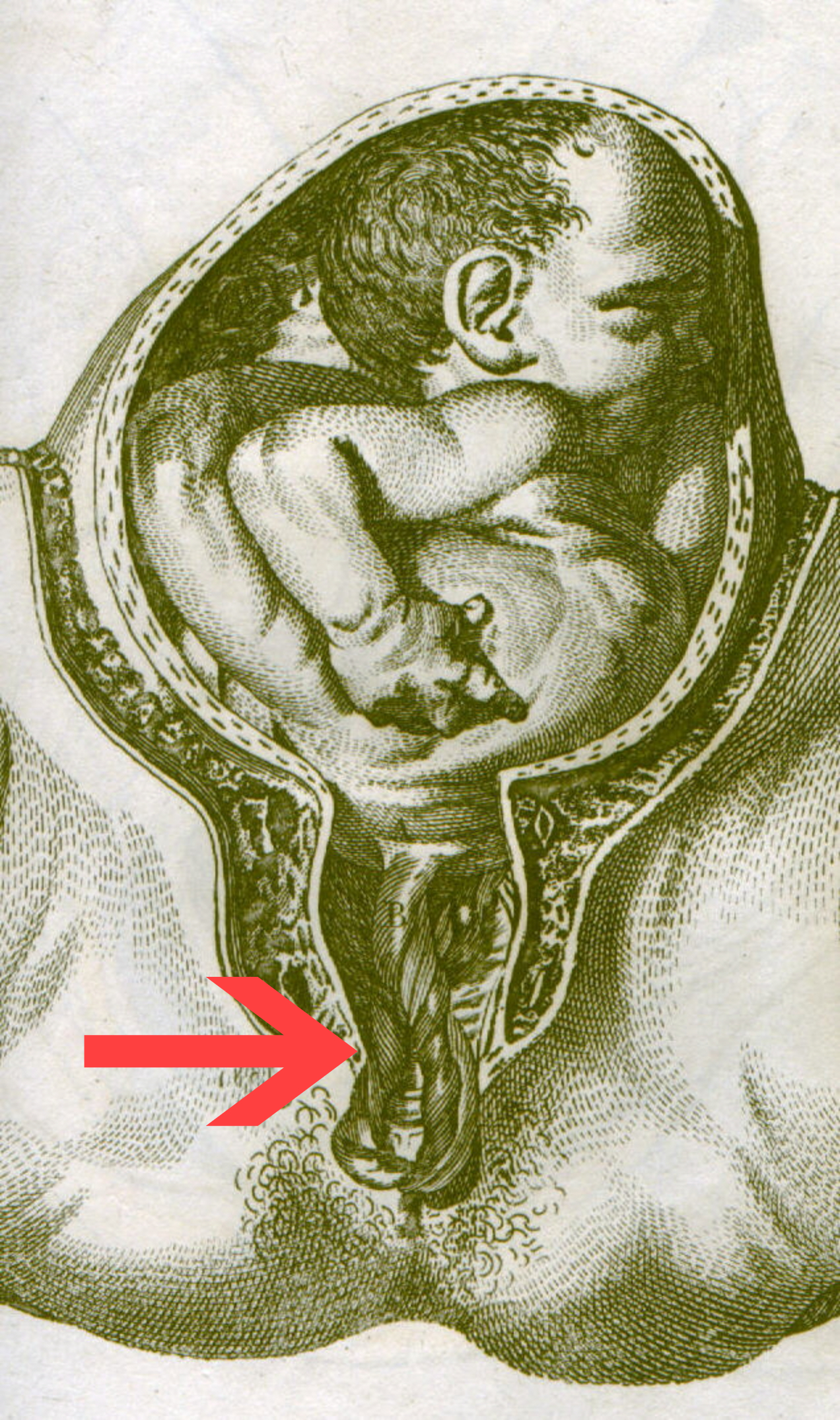
Special Situation: Cord Prolapse
Cord slips below presenting part. ACUTE hypoxia. OB EMERGENCY.
Immediate Actions:
1. Call for Help. 2. Manual Elevation: Lift head off cord. DO NOT REMOVE HAND. 3. Position: Knee-chest / Trendelenburg. 4. Immediate CS.
Summary & Documentation
Key Takeaways
• Use for induction/augmentation, not routine labor. • Strict ANTT is mandatory. • Ensure engagement to avoid cord prolapse. • Control fluid release carefully.
Note Documentation
• Time & Indication • FHR (Before & After) • Fluid characteristics • Consent & Tolerance
- amniotomy
- obstetrics
- labor-and-delivery
- medical-guidelines
- nursing-education
- clinical-protocols