
Elephantiasis: Lymphatic Filariasis Causes and Treatments
Explore a comprehensive guide to Elephantiasis (Lymphatic Filariasis), covering its causes, clinical complications, WHO drug treatments, and global elimination efforts.
ELEPHANTIASIS
Lymphatic Filariasis — Causes, Complications, Treatment & Epidemiology
A Comprehensive Overview
What is Elephantiasis?
Lymphatic Filariasis (LF)
Wuchereria bancrofti
infected mosquitoes
blockage and swelling
Asymptomatic → Acute → Chronic
Wuchereria bancrofti microfilaria (microscopy)
Potential Complications
Lymphoedema
Chronic tissue swelling of limbs, breasts, genitals
🦵
Tropical Pulmonary Eosinophilia
Coughing, breathing difficulty, elevated white blood cells
🫁
Hydrocele
Scrotal swelling affecting ~25 million men
💧
Recurrent Bacterial Infections
Compromised immunity leads to repeated skin infections
🦠
Psychosocial Impact
Social stigma, depression, loss of income, poverty cycle
🧠
Treatment & Management
Drug Therapies
DEC (Diethylcarbamazine)
Drug of choice, 6 mg/kg/day
Ivermectin
Used in onchocerciasis co-endemic areas
Albendazole
Combined with DEC or ivermectin in MDA
Doxycycline (4–6 weeks)
May stabilize lymphedema
Other Management
Complex Decongestive Physiotherapy (CDP)
Limb elevation & compression bandaging
Hygiene, skin care & wound management
Exercise & self-care routines
Hydrocelectomy (surgery) for hydrocele
VACCINATION & CONTROL PROGRAMS
No Current Vaccine
No licensed human vaccine exists. Multivalent vaccine candidates
(rBmHSP + rBmALT-2)
~90% protection
in mouse models.
Identified as a critical research need.
Mass Drug Administration (MDA)
WHO recommends annual MDA to all at-risk populations. Regimens:
DEC + Albendazole
(areas without onchocerciasis)
Ivermectin + Albendazole
(areas with onchocerciasis)
Triple Therapy (IDA)
DEC + Ivermectin + Albendazole
Conducted for 4–6 years minimum
Vector Control
Complementary vector control measures to reduce transmission:
Insecticide-treated bed nets
Indoor residual spraying
Personal protection measures
Xenomonitoring of mosquitoes
Tracking infection in vector populations
WHO'S GLOBAL PROGRAMME TO ELIMINATE LF (GPELF)
Launched 2000
Epidemiology — Global Burden
657 Million
people in 39 countries still at risk (2023)
51 Million
currently infected individuals
40 Million
living with chronic manifestations (lymphoedema/hydrocele)
74%
decline in prevalence since 2000
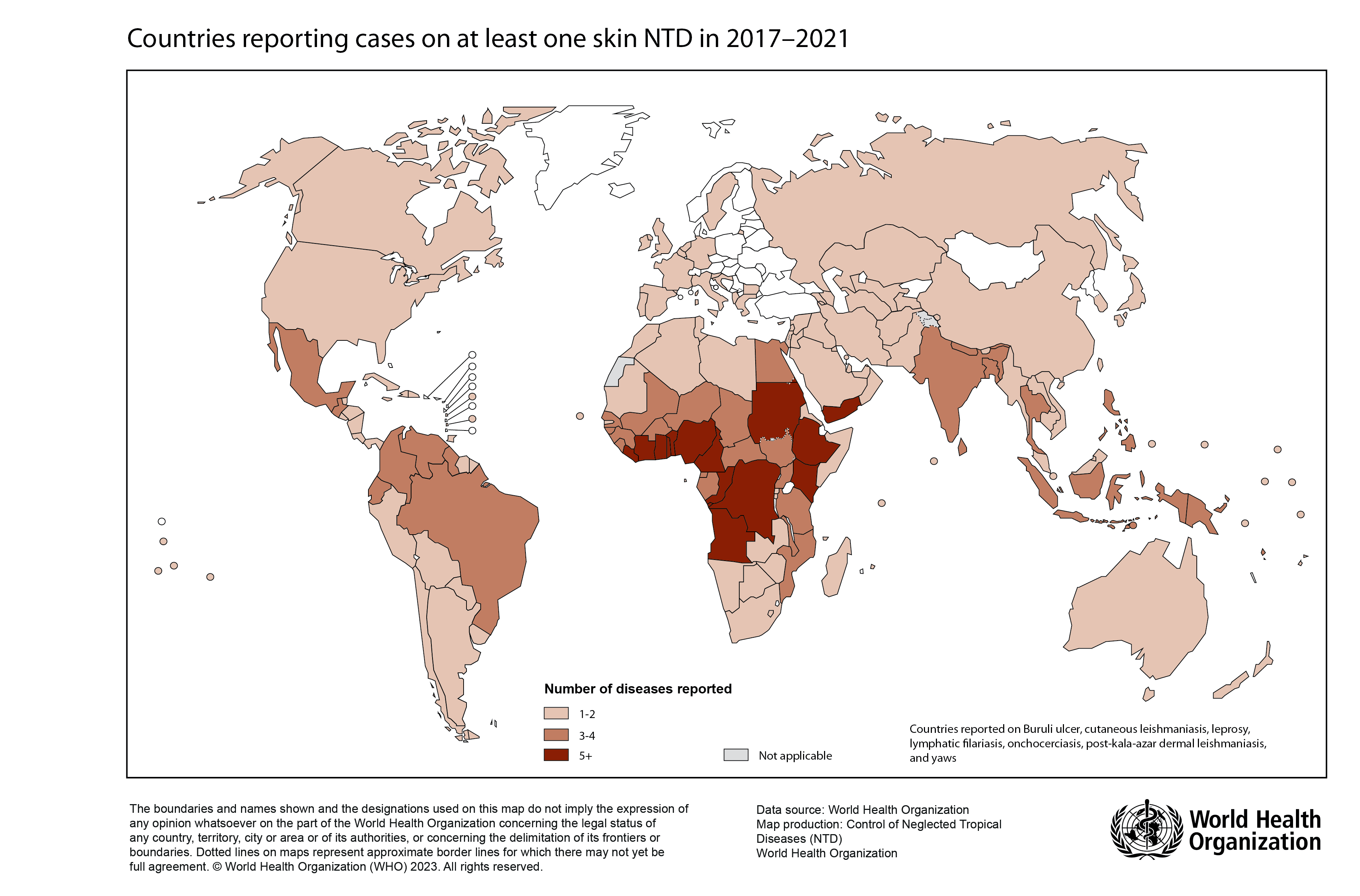
Geographic Distribution
<strong style="color: white; font-weight: 600;">90% of cases:</strong> Wuchereria bancrofti
Endemic in Asia, Sub-Saharan Africa, Caribbean, South America
<strong style="color: white; font-weight: 600;">India:</strong> 345 endemic districts; only 106 passed elimination surveys
<strong style="color: white; font-weight: 600;">Resurgence risk:</strong> post-elimination clusters detected (Futuna, 2024)
Endemic Countries — WHO
21 countries have achieved elimination as a public health problem • 871 million no longer require mda
Pathogen & Disease Images
Wuchereria bancrofti — Microfilariae (Light Microscopy)
Microfilaria — Unstained Blood Smear
Lymphoedema of Lower Limbs — Clinical Presentation
Key Takeaways
Caused by <i>Wuchereria bancrofti</i> — transmitted by infected mosquitoes
Complications: lymphoedema, hydrocele, pulmonary eosinophilia & psychosocial harm
Treatment: DEC, ivermectin & albendazole — no human vaccine yet available
WHO MDA program has reduced prevalence by 74% since year 2000
657 million still at risk — WHO targets full elimination by 2030
Source: World Health Organization (WHO) | 2023–2024 Data
- elephantiasis
- lymphatic-filariasis
- wuchereria-bancrofti
- global-health
- tropical-medicine
- public-health
- who