
Lymphatic Filariasis (Elephantiasis): Causes & Treatment
Explore the transmission, symptoms, risk factors, and WHO elimination strategies for Lymphatic Filariasis and Elephantiasis in this medical overview.
Neglected Tropical Disease
ELEPHANTIASIS
Lymphatic Filariasis — Disease Overview
Transmission · Symptoms · Treatment · Epidemiology
TRANSMISSION
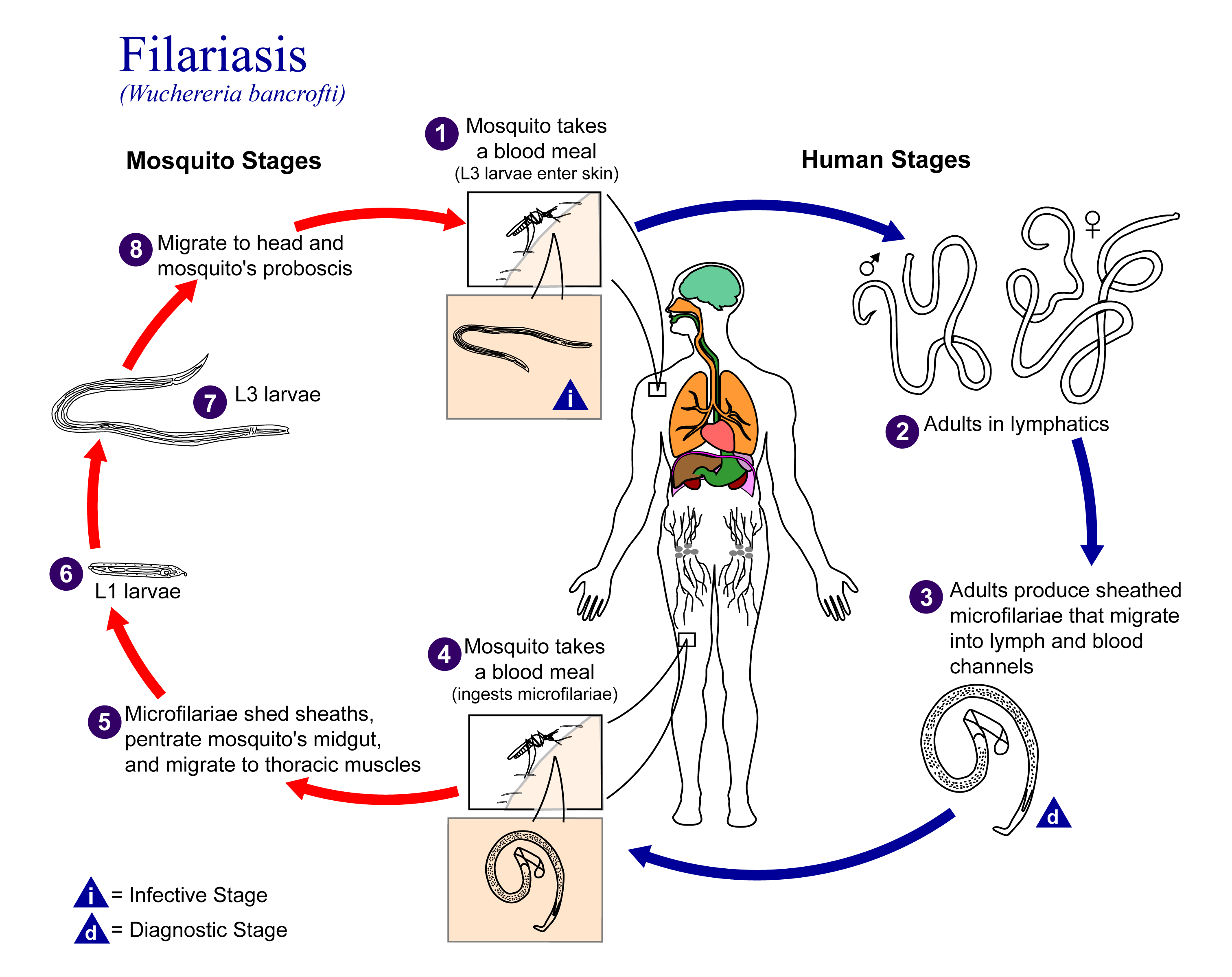
The disease is caused by parasitic filarial worms (<strong>Wuchereria bancrofti</strong> — 90% of cases, <strong>Brugia malayi</strong>, <strong>Brugia timori</strong>).
It is transmitted <span style="color: #0ecfca; font-weight: 700;">ONLY through mosquito bites</span> (NOT person to person).
Infected person has microfilariae (immature larvae) circulating in the blood.
Mosquito (Culex, Anopheles, Aedes, or Mansonia) bites infected person, ingesting microfilariae.
Microfilariae develop into infective 3rd-stage larvae inside the mosquito (10–14 days).
Mosquito bites a new human host — larvae enter through the bite wound.
Larvae migrate to lymphatic vessels and mature into adult worms (3–12 months).
Adult female worms release millions of microfilariae into the bloodstream — cycle repeats.
Repeated bites over months/years are typically required for infection. Microfilariae show <span style="color: #0ecfca; font-weight: 600;">NOCTURNAL PERIODICITY</span> — peak in bloodstream at night.
Incubation Period
The incubation period is the time between exposure to the pathogen and the onset of symptoms.
Mosquito Bite
Day 0
Larvae Develop in Mosquito
10–14 Days
Worms Mature in Host
3–12 Months
Symptoms Appear
Months to Years
Adult worms live 5–8 years inside the host, continuously releasing microfilariae
<span style="color: #0ecfca; font-weight: 700;">~66%</span> of infected people remain completely <span style="color: #0ecfca; font-weight: 700;">ASYMPTOMATIC</span> — yet still suffer hidden lymphatic and kidney damage
Microfilariae show <span style="color: #0ecfca; font-weight: 700;">NOCTURNAL PERIODICITY</span> — peak concentration in blood occurs at night
<span style="color: #0ecfca; font-weight: 700;">Silent progression</span> — most infected individuals are unaware they carry the parasite.
Disease Progression
SYMPTOMS
PHASE 1 — ASYMPTOMATIC (≈66% of cases)
No visible symptoms
Hidden lymphatic and kidney damage
Immune system changes occurring silently
PHASE 2 — ACUTE SYMPTOMS
Fever and skin inflammation
Lymphangitis (inflammation of lymph vessels)
Lymphadenopathy (enlarged lymph nodes)
Pain in limbs/genitals; acute episodes typically last 4–7 days
PHASE 3 — CHRONIC SYMPTOMS
Lymphedema — severe tissue swelling of arms, legs, genitals, and breasts
Elephantiasis — extreme skin thickening with pitted, hardened texture
Hydrocele — fluid accumulation causing scrotal swelling (in men)
Tropical Pulmonary Eosinophilia — rare condition marked by cough and wheezing
Secondary bacterial or fungal infections can severely worsen the condition
Lymphatic Filariasis · Clinical Manifestations · Pathophysiology
Risk Factors
Geographic Location
Living in or travelling to endemic tropical/subtropical regions: Sub-Saharan Africa, South/Southeast Asia (India, Bangladesh, Indonesia), Pacific Islands, Caribbean, and parts of South America.
Repeated Mosquito Exposure
Frequent, prolonged bites over months or years in endemic areas; outdoor exposure at night during peak mosquito activity.
Childhood Infection
Infection during childhood leads to significantly more severe long-term lymphatic dysfunction and tissue damage.
Poverty & Poor Housing
Limited access to insecticide-treated bed nets, poor sanitation, and open water sources providing prime mosquito breeding grounds.
Lack of Preventive Treatment
Not participating in widespread mass drug administration (MDA) programs increases individual and community risk.
Weakened Immune System
Conditions that compromise the immune system broadly increase susceptibility and greatly accelerate the severity of contraction.
Secondary Bacterial Infections
Poor wound care and hygiene lead to recurrent bacterial infections, physically worsening lymphedema and the hardening of tissues.
Elephantiasis · Lymphatic Filariasis · Disease Mechanics
Potential Complications
Permanent Lymphedema
Irreversible swelling of limbs, genitals, or breasts; progressive and disabling
Elephantiasis
Extreme skin thickening and hardening; loss of limb function; severe disfigurement
Hydrocele
Chronic fluid build-up in the scrotum; affects millions of men worldwide
Recurrent Bacterial & Fungal Infections (ADLA)
Secondary infections accelerate lymphatic damage; fever, pain, skin breakdown
Tropical Pulmonary Eosinophilia (TPE)
Lung involvement: chronic cough, wheezing, interstitial lung disease if untreated
Kidney Damage
Subclinical renal impairment: haematuria and proteinuria from microfilariae
Psychosocial Impact
Severe stigma, social isolation, depression, inability to work; profound socioeconomic burden
Reduced Immune Function
Increased vulnerability to other infections
<span style="color: #0ecfca; font-weight: 800; font-size: 32px;">~25 million</span> men affected by hydrocele <span style="color: rgba(14, 207, 202, 0.4); font-size: 28px;">|</span> <span style="color: #0ecfca; font-weight: 800; font-size: 32px;">~15 million</span> people living with lymphedema globally
Treatment & Management
Drug Treatments (Antiparasitic)
Morbidity Management & Other Therapies
Clinical Care · Intervention Protocols · Patient Support
Vaccination & Control Programs
Vaccination
No vaccine currently exists for lymphatic filariasis.
Research is ongoing but limited; there is no approved immunisation program.
NO VACCINE AVAILABLE
Control Programs
WHO Global Programme to Eliminate Lymphatic Filariasis (GPELF) — launched 2000
Eliminate LF as a public health problem by 2030
Mass Drug Administration (MDA)
Annual single-dose treatment of entire at-risk populations in endemic areas regardless of infection status; regimens: IDA, or ivermectin + albendazole.
Morbidity Management & Disability Prevention (MMDP)
Implementing hygiene protocols, delivering care packages, and providing surgery access for existing cases.
Vector Control
Insecticide-treated nets (ITNs), larval management, spraying.
Surveillance
Rigorous post-MDA monitoring to confirm elimination.
Community Ed
Local health promotion and community engagement.
Over 9.7 billion treatments delivered • 21+ countries achieved elimination • ~$100 billion in economic losses averted
EPIDEMIOLOGY
657 Million
People in 39 countries requiring preventive chemotherapy (2023)
36 Million
People with chronic disease (lymphedema or hydrocele)
15 Million
People with lymphedema globally
25 Million
Men with hydrocele globally
Pathogen & Disease Images
Wuchereria bancrofti — the filarial worm responsible for ~90% of lymphatic filariasis cases (CDC)
Life cycle of W. bancrofti — from mosquito vector to human host (CDC/Wikipedia)
Clinical elephantiasis — severe lymphedema of the lower limbs
Wuchereria bancrofti adult worms are thread-like, 4–10 cm long. Microfilariae are ~250 μm. Adult worms live 5–8 years in the lymphatic system.
- elephantiasis
- lymphatic-filariasis
- tropical-disease
- mosquito-borne-diseases
- public-health
- epidemiology