Heart Failure: Clinical Framework for Junior Doctors
A comprehensive guide for JMOs on diagnosing and managing heart failure, including aetiology, pathophysiology, investigations, and the 4 pillars of treatment.
CASE-BASED APPROACH · JMO LEVEL
Heart Failure
A Clinical Framework for Junior Doctors
PRESENTING CASE
72M | SOB × 3 days, orthopnoea, PND
Bilateral leg swelling
Hypertension, Ischaemic Heart Disease
What are your top differentials?
Heart Failure | JMO Teaching Session | 2026
SLIDE 2 · DIFFERENTIALS
Acute Dyspnoea + Oedema
🔴 CARDIAC
Heart Failure (acute decompensation)
ACS → causing HF
Arrhythmia (AF with RVR)
🟠 RESPIRATORY
Pneumonia
COPD exacerbation
Pulmonary Embolism
🟡 OTHER
Renal failure (fluid overload)
Liver disease (ascites, oedema)
Hypoalbuminaemia
💡 Clue toward HF: Orthopnoea + PND + bilateral oedema → classic constellation
Heart Failure | JMO Teaching Session | 2026
SLIDE 3 · AETIOLOGY
Causes of Heart Failure
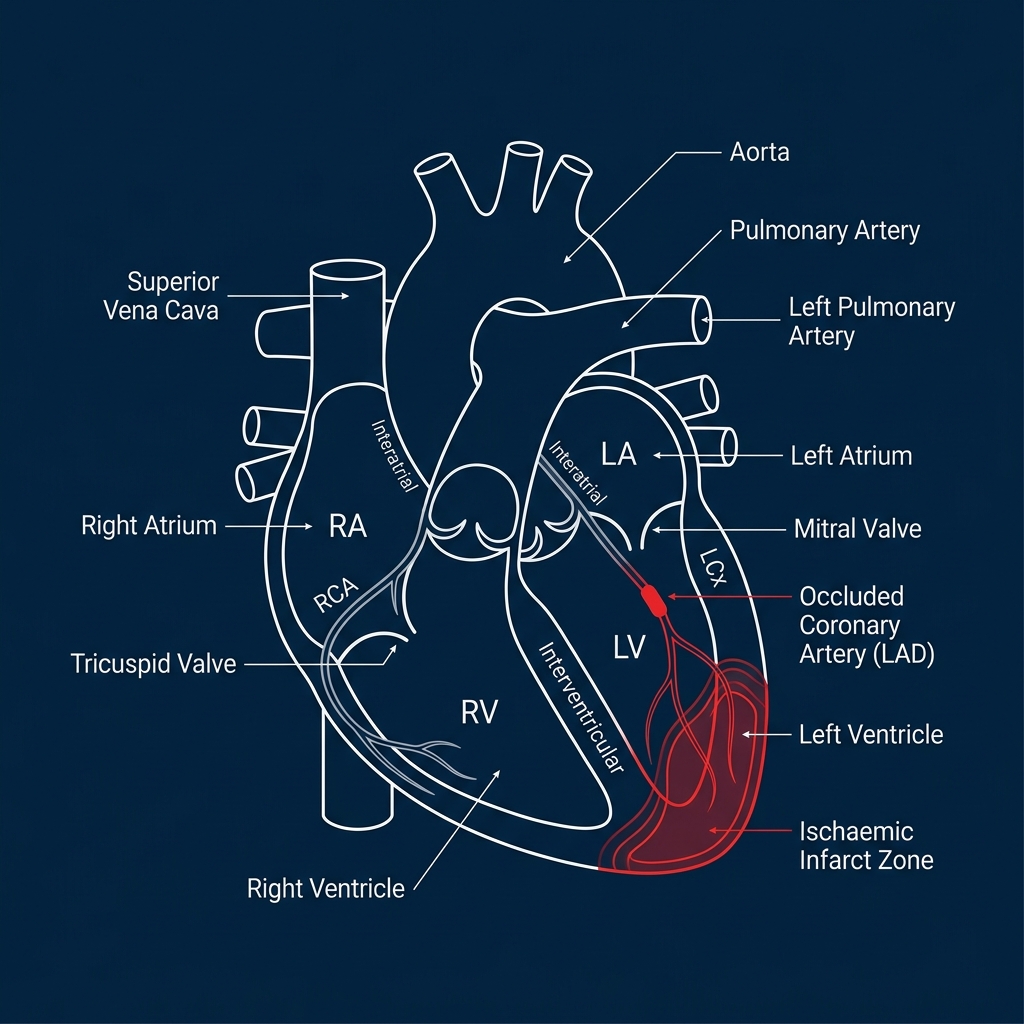
ISCHAEMIC
Most Common Cause
CAD / prior MI → myocardial damage
PRESSURE OVERLOAD
Hypertension
Aortic stenosis
VOLUME OVERLOAD
Mitral regurgitation
Aortic regurgitation
MYOCARDIAL DISEASE
Dilated cardiomyopathy
Hypertrophic cardiomyopathy
Myocarditis
OTHER CAUSES
Arrhythmias (AF, VT)
Alcohol / cardiotoxic drugs
Thyroid disease (hypo/hyper)
Heart Failure | JMO Teaching Session | 2026
SLIDE 4 · PATHOPHYSIOLOGY & FEATURES
Pathophysiology + Clinical Features
⚙️ PATHOPHYSIOLOGY
↓ Cardiac Output
↑ RAAS Activation
Fluid Retention
↑ Preload & Afterload
Further ↓ in cardiac output (vicious cycle)
Compensatory → eventually maladaptive
😮💨 SYMPTOMS
Dyspnoea on exertion
Orthopnoea (↑ pillows)
Paroxysmal nocturnal dyspnoea (PND)
Fatigue / reduced exercise tolerance
Ankle swelling
Abdominal bloating (RHF)
🩺 SIGNS
Raised JVP
Bibasal crackles
Peripheral / pitting oedema
S3 gallop (ventricular filling)
Displaced apex beat
Hepatomegaly (RHF)
Ascites (severe)
💡 Think: Fluid overload (congestion) + Poor perfusion (low output) — both can coexist
Heart Failure | JMO Teaching Session | 2026
SLIDE 5 · INVESTIGATIONS
Investigations – What You Actually Do
📋 BEDSIDE
Vital signs (HR, BP, SpO2, RR)
ECG → ischaemia, AF, LVH, LBBB
Fluid balance chart
Daily weight
🩸 BLOODS
BNP / NT-proBNP ↑↑ (key marker)
UEC → renal function, K+
LFTs → hepatic congestion
Troponin → rule out ACS trigger
FBC → anaemia as trigger
TFTs → thyroid cause
BSL → diabetic cardiomyopathy
🖼️ IMAGING
CXR → pulmonary oedema, cardiomegaly, Kerley B lines, pleural effusions
Echocardiogram ⭐ GOLD STANDARD
Echo: EF → HFrEF (<40%) vs HFpEF (≥50%)
Echo: valve function + wall motion
🌟 Echo = Gold Standard for Diagnosis | ⚠️ Normal BNP makes HF diagnosis unlikely
Heart Failure | JMO Teaching Session | 2026
SLIDE 6 · MANAGEMENT
Management – Acute & Chronic
🔴 ACUTE DECOMPENSATED HF (Ward)
Immediate Actions
Sit upright (reduces preload)
Oxygen if SpO2 <94%
IV access + monitoring
Medications
IV Frusemide ⭐ (key — titrate to urine output)
GTN infusion if hypertensive
Consider CPAP/BiPAP if respiratory distress
Monitor
Urine output hourly
Daily weight
Electrolytes (K+, Cr)
Fluid balance
🟢 CHRONIC HF – 4 PILLARS (HFrEF)
1️⃣ ACEi / ARNI (e.g. Ramipril / Sacubitril-Valsartan) — reduces afterload, mortality benefit
2️⃣ Beta-blocker (e.g. Carvedilol, Bisoprolol) — reduces HR, remodelling
3️⃣ MRA (e.g. Spironolactone) — anti-aldosterone, reduces fluid
4️⃣ SGLT2 Inhibitor (e.g. Empagliflozin, Dapagliflozin) — newest, strong mortality benefit
⚕️ Non-Pharmacological
Fluid restriction (1.5L/day)
Salt restriction
Daily weights at home
Influenza + pneumococcal vaccination
Cardiac rehabilitation
Heart Failure | JMO Teaching Session | 2026
SLIDE 7 · TRIGGERS & COMPLICATIONS
Triggers, Complications & Red Flags
TRIGGERS
Infection / Sepsis
Acute Coronary Syndrome
Arrhythmia (AF with RVR)
Medication non-compliance
Uncontrolled hypertension
Renal failure
Anaemia
NSAIDs / CCBs
COMPLICATIONS
Acute pulmonary oedema
Cardiogenic shock
AF / VT / VF
Cardiorenal syndrome
Hepatic congestion
DVT / Pulmonary Embolism
Depression & poor QoL
RED FLAGS
(Escalate Now)
SBP < 90 mmHg
Rising creatinine
Urine output < 0.5 mL/kg/hr
Persistent hypoxia
Altered consciousness
New arrhythmia
Call Senior / ICU Early
Finding and fixing the trigger is what prevents the next admission
Heart Failure | JMO Teaching Session | 2026
SLIDE 8 · CASE RESOLUTION
Back to Our Patient
CASE RECAP
<span style="color:#FFFFFF; font-weight:700;">72M</span> <span style="color:rgba(255,255,255,0.3); margin:0 8px;">|</span> SOB × 3 days <span style="color:rgba(255,255,255,0.3); margin:0 8px;">|</span> Orthopnoea, PND <span style="color:rgba(255,255,255,0.3); margin:0 8px;">|</span> Bilateral oedema <span style="color:rgba(255,255,255,0.3); margin:0 8px;">|</span> <span style="color:#C77DFF; font-weight:600;">PMHx:</span> HTN, IHD
LIKELY DIAGNOSIS
<strong style="color: #FFFFFF; font-weight: 700;">Acute Decompensated Heart Failure</strong>
Most likely <strong style="color: #FFB703;">ISCHAEMIC</strong> cause <span style="color: #A0A5AA; font-size: 22px;">(IHD background)</span>
<span style="color:#E0E1E2;">Possible trigger: <span style="color: #FFB703;">? Infection</span>, <span style="color: #FFB703;">? ACS</span>, <span style="color: #FFB703;">? Non-compliance</span></span>
YOUR PLAN
Sit up + O₂ if hypoxic
IV Frusemide (40–80mg) stat
ECG → rule out ACS trigger
Bloods: Troponin, BNP, UEC, FBC
CXR → confirm pulmonary oedema
Echo → confirm HF, assess EF
Identify + treat the trigger
Monitor: UO, weight, electrolytes
Refer Cardiology
Treat the fluid — but always ask: WHY did they decompensate?
Heart Failure | JMO Teaching Session | 2026
SLIDE 9 · TAKE HOME
Key Take-Home Points
🩺
Think Heart Failure in ANY patient with SOB + bilateral oedema
⚡
Always rule out an ACS trigger — troponin + ECG in every patient
🔬
Echo is the gold standard — confirms diagnosis and guides management
💧
Treat fluid overload early — IV frusemide and monitor response
🔍
Identify and fix the trigger — this prevents the next admission
In heart failure, treating the fluid is important — but finding and fixing the trigger is what prevents the next admission.
— The clinical principle to carry through your career
Heart Failure | JMO Teaching Session | 2026
- heart-failure
- medical-education
- junior-doctor-teaching
- cardiology
- hfref-management
- clinical-framework